
Jorge I. de la Torre, MD, FACS
- Professor of Surgery
- Chief, Division of Plastic Surgery
- University of Alabama at Birmingham School of Medicine
- Section Chief, Plastic Surgery Section
- Birmingham VA Medical Center
- Birmingham, Alabama
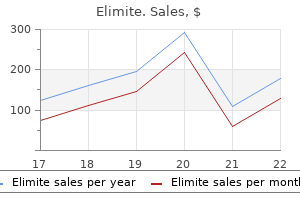
Publication bias assessment and analysis was not performed since there is very few studies included acne on neck buy cheap elimite on line. Summary of risk of bias assessment + denotes low risk; denotes high risk; blank denotes unclear risk skin care di jakarta purchase cheap elimite online. Also acne treatment for teens buy 30 gm elimite with mastercard, there is a high risk for reporting bias acne inversa elimite 30gm fast delivery, since not all outcomes were properly reported acne in your 30s buy elimite 30gm mastercard. Table 13) has a high risk for other bias acne 9 month old buy elimite toronto, since the study is sponsored by a pharmaceutical company. Meanwhile, it has low risk for selection, performance, detection, and attrition bias since randomization and blinding were ensured through its design, and there is a low number of attrition. Attrition bias Incomplete outcome Low Risk Low number of attrition in the data continuation phase is not enough to have a clinically relevant effect Reporting bias Selective reporting High Risk the article reported most pre-specified outcomes; however, some are not presented in proper tables, making it harder for readers to easily read the results. Other bias Other sources of High risk Study sponsored by a bias pharmaceutical company which markets the drug of interest. High Risk High number of attrition in the Attrition bias Incomplete outcome continuation phase is enough data to have a clinically relevant effect Low Risk the article reported all Reporting bias Selective reporting pre-specified outcomes and presented in proper tables, making it easier for readers to easily read the results. High risk Study sponsored by a Other bias Other sources of bias pharmaceutical company which markets the drug of interest. Based on the judgment of the reviewers, there is high risk for attrition, reporting, and other bias. This is because there is a high number of attrition in the continuation phase, the imputation method used was the last-observation-carried-forward imputation, and the study is sponsored by a pharmaceutical company. Nevertheless, blinding and randomization was ensured by the design of the study, thus making it low risk for selection, performance, and detection bias. Allocation Unclear There was no mention of concealment risk concealment of allocation of patients. Performance bias Blinding of Low risk the study has a double-blind participants and design. However, caution should be taken in interpreting these results since there is a risk for bias, particularly in terms of attrition and reporting bias. No conclusion on comparative clinical benefit in terms of efficacy or safety can be drawn in comparison with insulin since there was no available data. Model Parameters A systematic literature search was carried out to identify transition probabilities, measures of clinical effect, and health utilities. Clinical Effectiveness Details of the systematic review conducted were presented in depth in the previous chapter. The evaluation assumes a class effect since there are no studies on the subgroup of interest using gliclazide, the drug more commonly used in the Philippines. Because no local weights were available at the time of the study, utility values were no longer derived to Philippine values. All inputs were reported in terms of annual cost per patient, based on assumptions and recommendations from key informants. As validated by an endocrinologist, the dose for insulin was assumed to not change regardless of kidney function. The components of the maintenance costs were also validated by an endocrinologist, and all drugs were assumed to be taken once daily for a year. Estimating the monitoring cost per treatment arm required several assumptions and utilised various data sources. The cost of an HbA1c blood test was based on a nationally representative health facility survey conducted in 2016. Summary of parameters Parameters Estimated value Distribution Reference Baseline parameters Discount rate outcomes 3. Sitagliptin is also the most expensive option out of the 3 drugs, with a price 3 times more expensive than insulin and over 12 times of the price of gliclazide. Even when monitoring costs are factored in, with insulin having the highest amount, the high unit price of sitagliptin makes the total treatment cost still the most expensive intervention. The same can be said for the discount rates on costs and outcomes used, which had no effect on the overall ratio. Parameter Uncertainty Given that the price of the sitagliptin is the largest determinant for cost effectiveness, a one-way scenario analysis was conducted using different costs for sitagliptin based on possible price discounts offers. A higher discount is needed when compared against gliclazide, as their monitoring costs are equal. A probabilistic sensitivity analysis using Monte Carlo simulation of 10, 000 iterations was carried out on all cost components and treatment effects. They were transformed into their probabilistic values based on their assumed distributions. Results of the simulation for sitagliptin versus gliclazide and insulin are presented in Figure 6A. Eighty-four percent of the trials versus gliclazide fell within the northeast quadrant of the cost effectiveness plot, while the analysis against insulin yielded 62% in the same area ure 6B). Budget Impact Analysis An additional analysis on budget impact based on existing prevalence data and assumptions on utilization was carried out to support the analysis. Due to the limited treatments available for this subpopulation, this drug was considered for review as it may have a potential role as well as serve as an affordable treatment due to the small population included. First, the assessment heavily relied on the limited published clinical trials obtained from 4 databases where only English articles were considered. Furthermore, the 3 trials obtained, all of which were funded by pharmaceutical industries, used glipizide instead of gliclazide as the active comparator. Third, the assessment also considered local cost estimates of treatment and monitoring costs from available databases, selected local stores in Bambang, Sta. Acquisition costs of sitagliptin compared to gliclazide is much larger, which would be challenging to show value for money due to the availability of generic versions of the latter. Due to this limitation, the local cost estimates might not be representative of the actual cost. Fourth, utility and disutility values were based on studies conducted in other countries, which mostly involved American and European populations. Based on these limitations, the findings of our review must be interpreted with caution. Given these limitations, the findings would remain the same due to the following reasons. One-way sensitive analyses showed that the major drivers of the assessment were the safety profile of the drugs. Overall conclusion While sitagliptin provides better safety outcomes in terms of reduced risk of severe hypoglycemia, this added value is not justified by the difference in price when compared to the benefits and costs of gliclazide and insulin. Epidemiology, presentation, and diagnosis of type 2 diabetes mellitus in children and adolescents UpToDate [Internet]. Clinical Practice Guidelines Chronic Kidney Disease in Diabetes Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Chronic kidney disease in patients with diabetes mellitus type 2 or hypertension in general practice. Challenges in achieving optimal glycemic control in type 2 diabetes patients with declining renal function: the Southeast Asia perspective. Treatment of type 2 diabetes in chronic kidney disease: a case for linagliptin in the treatment of diabetes in severe renal impairment. Behavioral science research in diabetes: Lifestyle changes related to obesity, eating behavior, and physical activity [Internet]. Adherence to Self-Care Behavior in Patients Diagnosed with Type 2 Diabetes Mellitus in the Outpatient Department of the Philippine General Hospital. Pill Burden, Adherence, Hyperphosphatemia, and Quality of Life in Maintenance Dialysis Patients. Pharmaceutical intervention on the therapeutic adherence in patients with chronic renal disease. Adherence to Antihypertensive Agents and Blood Pressure Control in Chronic Kidney Disease. Adherence to insulin and its association with glycaemic control in patients with type 2 diabetes. Adherence, Persistence, and Health Care Costs for Patients Receiving Dipeptidyl Peptidase-4 Inhibitors. Assessing oral medication adherence among patients with type 2 diabetes mellitus treated with polytherapy in a developed Asian community: a cross-sectional study. Adherence, persistence, and treatment discontinuation with sitagliptin compared with sulfonylureas as add-ons to metformin: A retrospective cohort database study. Refill compliance in type 2 diabetes mellitus: A predictor of switching to insulin therapy Prevalence and Predictors of Medication Non-Adherence in Patients of Chronic Kidney Disease: Evidence from A Cross Sectional Study. Medication adherence and achievement of glycaemic targets in ambulatory type 2 diabetic patients. Nonadherence and factors affecting adherence of diabetic patients to anti-diabetic medication in Assela General Hospital, Oromia Region, Ethiopia. Antidiabetic medication adherence and associated factors among patients in Botswana; implications for the future. Medication Adherence in Patients with Diabetes and Dyslipidemia: Associated Factors and Strategies for Improvement. Management of diabetes mellitus in individuals with chronic kidney disease: therapeutic perspectives and glycemic control. Management of hyperglycemia in patients with type 2 diabetes and pre-dialysis chronic kidney disease or end-stage renal disease UpToDate [Internet]. Impact of diabetic nephropathy on pharmacodynamic and Pharmacokinetic properties of insulin in type 1 diabetic patients. Pharmacokinetics of insulin aspart in obesity, renal impairment, or hepatic impairment. Insulin requirements in patients with diabetes and declining kidney function: differences between insulin analogues and human insulin Diabetic Kidney Disease: Hyperglycemia Management Renal and Urology News [Internet]. Current therapeutic approaches in the management of hyperglycemia in chronic renal disease. Day-to-Day Variation of Insulin Requirements of Patients With Type 2 Diabetes and End-Stage Renal Disease Undergoing Maintenance Hemodialysis. Insulin therapy during peritoneal dialysis: pros and cons of various forms of administration. Reviews: Use of Insulin and Oral Hypoglycemic Medications in Patients with Diabetes Mellitus and Advanced Kidney Disease. Health behaviors and risk factors associated with chronic kidney disease in Korean patients with diabetes: the fourth Korean national health and nutritional examination survey. Glucose-lowering drugs in patients with chronic kidney disease: a narrative review on pharmacokinetic properties. Severe relapsing sulphonylurea-induced hypoglycaemia: a diagnostic and therapeutic challenge. A 16-week study to compare the effect of vildagliptin versus gliclazide on postprandial lipoprotein concentrations and oxidative stress in patients with type 2 diabetes inadequately controlled with metformin monotherapy. The self management experience of patients with type 2 diabetes and chronic kidney disease: A qualitative study. Safety and efficacy of sitagliptin in patients with type 2 diabetes and chronic renal insufficiency. Glycated Albumin Is a Better Glycemic Indicator than Glycated Hemoglobin Values in Hemodialysis Patients with Diabetes: Effect of Anemia and Erythropoietin Injection. Glycated Albumin and Risk of Death and Hospitalizations in Diabetic Dialysis Patients. While guidelines are useful aids to assist providers in determining appropriate practices for many patients with specific clinical problems or prevention issues, guidelines are not meant to replace the clinical judgment of the individual provider or establish a standard of care. The recommendations contained in the guidelines may not be appropriate for use in all circumstances. A decision to adopt any particular recommendation must be made by the provider in light of the circumstances presented by the individual patient. Because glimepiride has been added to the Beers Glimepiride was not on the Beers list and was list of drugs to avoid in the elderly, sulfonylurea the preferred sulfonylurea regardless of patient recommendations are now as follows: age. Prevention Studies have shown that increasing physical activity and eating a healthy diet can significantly delay the onset of type 2 diabetes, including for patients diagnosed with impaired glucose tolerance. Studies have also shown that the use of metformin can delay the diagnosis of diabetes for patients with impaired glucose tolerance, but there is no evidence that metformin or any other medication leads to long-term better clinical outcomes prior to diagnosis of diabetes. Preventive Services Task Force (Siu 2015) recommends screening patients who are at increased risk for diabetes. If the decision is to screen, consider a frequency of every 3 years using either fasting plasma glucose or HbA1c. If they elect screening, these patients should be screened every 3 years using either fasting plasma glucose or HbA1c. Annual screening is recommended for women with a history of gestational diabetes (using HbA1c) and for men and women with impaired fasting blood glucose (using either fasting plasma glucose or HbA1c).
Depersonalization is a very common symptom in the general population and may contribute to neurological presentations described as dizziness acne red marks buy elimite 30 gm on-line, numbness acne under microscope buy 30gm elimite with mastercard, and forgetfulness acne zapping machine generic elimite 30 gm online, with the broad differential diagnoses that such symptoms encompass acne scar laser treatment discount 30 gm elimite with mastercard. Such self-induced symptoms may occur in the context of meditation and self-suggestion acne zapper zeno buy elimite 30 gm otc. Cross References Derealization; Dissociation Derealization Derealization skin care diet purchase elimite 30 gm line, a form of dissociation, is the experience of feeling that the world around is unreal. Cross References Alien hand, Alien limb; Intermanual conict Diamond on Quadriceps Sign Diamond on quadriceps sign may be seen in patients with dysferlinopathies (limb girdle muscular dystrophy type 2B, Miyoshi myopathy): with the knees slightly bent so that the quadriceps are in moderate action, an asymmetric diamond shaped bulge may be seen, with wasting above and below, indicative of the selectivity of the dystrophic process in these conditions. Cross Reference Calf head sign Diaphoresis Diaphoresis is sweating, either physiological as in sympathetic activation. Diaphoresis may be seen in syncope, delirium tremens, or may be induced by certain drugs. Anticholinergics decrease diaphoresis but increase core temperature, resulting in a warm dry patient. Forced vital capacity measured in the supine and sitting positions is often used to assess diaphragmatic function, a drop of 25% being taken as indicating diaphragmatic weakness. The spatial and temporal characteristics of the diplopia may help to ascertain its cause. Diplopia may be monocular, in which case ocular causes are most likely (although monocular diplopia may be cortical or functional in origin), or binoc ular, implying a divergence of the visual axes of the two eyes. With binocular diplopia, it is of great importance to ask the patient whether the images are sep arated horizontally, vertically, or obliquely (tilted), since this may indicate the extraocular muscle(s) most likely to be affected. Whether the two images are 108 Diplopia D separate or overlapping is important when trying to ascertain the direction of maximum diplopia. The effect of gaze direction on diplopia should always be sought, since images are most separated when looking in the direction of a paretic mus cle. Conversely, diplopia resulting from the breakdown of a latent tendency for the visual axes to deviate (latent strabismus, squint) results in diplopia in all directions of gaze. Examination of the eye movements should include asking the patient to look at a target, such as a pen, in the various directions of gaze (versions) to ascertain where diplopia is maximum. Then, each eye may be alternately covered to try to demonstrate which of the two images is the false one, namely that from the non-xing eye. Manifest squints (heterotropia) are obvious but seldom a cause of diplopia if long-standing. Transient diplopia (minutes to hours) suggests the possibility of myasthenia gravis. Divergence of the visual axes or ophthalmoplegia without diplopia sug gests a long-standing problem, such as amblyopia or chronic progressive external ophthalmoplegia. Cross References Motor neglect; Neglect Disc Swelling Swelling or oedema of the optic nerve head may be visualized by ophthal moscopy. It produces haziness of the nerve bre layer obscuring the underlying vessels; there may also be haemorrhages and loss of spontaneous retinal venous pulsation. Disc swelling due to oedema must be distinguished from pseudopapil loedema, elevation of the optic disc not due to oedema, in which the nerve bre layer is clearly seen. The clinical history, visual acuity, and visual elds may help determine the cause of disc swelling. The disinhibited patient may be inap propriately jocular (witzelsucht), short-tempered (verbally abusive, physically aggressive), distractible (impaired attentional mechanisms), and show emo tional lability. A Disinhibition Scale encompassing various domains (motor, intellectual, instinctive, affective, sensitive) has been described. Disinhibition is a feature of frontal lobe, particularly orbitofrontal, dysfunc tion. Cross References Attention; Emotionalism, Emotional lability; Frontal lobe syndromes; Witzelsucht Dissociated Sensory Loss Dissociated sensory loss refers to impairment of selected sensory modalities with preservation, or sparing, of others. Conversely, pathologies conned, largely or exclusively, to the dorsal columns (classically tabes dorsalis and subacute combined degenera tion of the cord from vitamin B12 deciency, but probably most commonly seen with compressive cervical myelopathy) impair proprioception, sometimes suffi cient to produce pseudoathetosis or sensory ataxia, whilst pain and temperature sensation is preserved. Small bre peripheral neuropathies may selectively affect the bres which transmit pain and temperature sensation, leading to a glove-and-stocking impair ment to these modalities. Neuropathic (Charcot) joints and skin ulceration may occur in this situation; tendon reexes may be preserved. Common in psychiatric disorders (depression, anxiety, schizophre nia), these symptoms are also encountered in neurological conditions (epilepsy, migraine, presyncope), conditions such as functional weakness and non-epilpetic attacks, and in isolation by a signicant proportion of the general population. Symptoms of dizziness and blankness may well be the result of dissociative states rather than neurological disease. The superior division or ramus supplies the superior rectus and levator palpebrae superioris muscles; the inferior division or ramus supplies medial rectus, inferior rectus and inferior oblique muscles. Isolated dys function of these muscular groups allows diagnosis of a divisional palsy and suggests pathology at the superior orbital ssure or anterior cavernous sinus. However, occasionally this division may occur more proximally, at the fascicu lar level. Although this can be done in a conscious patient focusing on a visual target, smooth pursuit eye movements may compensate for head turn ing; hence the head impulse test (q. The manoeuvre is easier to do in the unconscious patient, when testing for the integrity of brainstem reexes. In many elderly people the extensor tendons are prominent in the absence of signicant muscle wasting. Cross Reference Wasting Double Elevator Palsy this name has been given to monocular elevation paresis. It may occur in associ ation with pretectal supranuclear lesions either contralateral or ipsilateral to the paretic eye interrupting efferents from the rostral interstitial nucleus of the medial longitudinal fasciculus to the superior rectus and inferior oblique subnuclei. This syndrome has a broad differ ential diagnosis, encompassing disorders which may cause axial truncal muscle weakness, especially of upper thoracic and paraspinous muscles. Treatment of the underlying condition may be possible, hence investigation is mandatory. They occur sporadically or may be inherited in an autosomal dominant fashion, and are common, occurring in 2% of the population. Drusen are usually asymptomatic but can cause visual eld defects (typically an inferior nasal visual eld loss) or occasionally transient visual obscurations, but not changes in visual acuity; these require investigation for an alternative cause. When there is doubt whether papilloedema or drusen is the cause of a swollen optic nerve head, retinal uorescein angiography is required. Cross References Disc swelling; Papilloedema; Pseudopapilloedema; Visual eld defects 114 Dysarthria D Dynamic Aphasia Dynamic aphasia refers to an aphasia characterized by difficulty initiating speech output, ascribed to executive dysfunction. There is a reduction in spontaneous speech, but on formal testing there are no paraphasias, minimal anomia, pre served repetition, and automatic speech. A division into pure and mixed forms has been suggested, with additional phonological, lexical, syntactical, and articulatory impairments in the latter. Some authorities reserve the term for provoked positive sensory phenomena, as opposed to spontaneous sensations (paraesthesia). Dysaesthesia differs from paraesthesia in its unpleasant quality, but may overlap in some respects with allodynia, hyperalgesia, and hyper pathia (the latter phenomena are provoked by stimuli, either non-noxious or noxious). There are many causes of dysaesthesia, both peripheral (including small bre neuropathies, neuroma, and nerve trauma) and central. Dysaesthetic sensations may be helped by agents such as carbamazepine, amitriptyline, gabapentin, and pregabalin. Cross References Allodynia; Hyperalgesia; Hyperpathia; Paraesthesia Dysarthria Dysarthria is a disorder of speech, as opposed to language (cf. Dysarthria is a symptom, which may be caused by a number of differ ent conditions, all of which ultimately affect the function of pharynx, palate, tongue, lips, and larynx, be that at the level of the cortex, lower cranial nerve nuclei or their motor neurones, neuromuscular junction, or bulbar muscles them selves. Dysarthrias affect articulation in a highly reliable and consistent manner, the errors reecting the muscle group involved in the production of specic sounds. Dysdiadochokinesia is a sign of cerebellar dysfunction, especially hemi sphere disease, and may be seen in association with asynergia, ataxia, dysme tria, and excessive rebound phenomenon. Cross References Asynergia; Apraxia; Ataxia; Cerebellar syndromes; Dysmetria; Rebound phe nomenon Dysexecutive Syndrome the term executive function encompasses a range of cognitive processes includ ing sustained attention, uency and exibility of thought, problem-solving skills, 117 D Dysgeusia and planning and regulation of adaptive and goal-directed behaviour. Decits in these various functions, the dysexecutive syndrome, are typically seen with lateral prefrontal cortex lesions. Cross References Attention; Frontal lobe syndromes Dysgeusia Dysgeusia is a complaint of distorted taste perception. It may occur along with anosmia as a feature of upper respiratory tract infections and has also been described with various drug therapies, in psychiatric diseases, and as a feature of zinc deciency. The term may be qualied to describe a number of other syndromes of excessive movement. Cross Reference Alexia Dysmentia the term dysmentia has been suggested as an alternative to dementia, to emphasize the possibility of treating and preventing cognitive decline. Cross Reference Dementia Dysmetria Dysmetria, or past-pointing, is a disturbance in the control of range of move ment in voluntary muscular action and is one feature of the impaired checking response seen in cerebellar lesions (especially cerebellar hemisphere lesions). Dysmetria may also be evident in saccadic eye movements: hypometria (undershoot) is common in parkinsonism; hypermetria (overshoot) is more typical of cerebellar disease (lesions of dorsal vermis and fastigial nuclei). In cerebellar disorders, dysmetria reects the asynergia of coordinated muscular contraction. Cross References Asynergia; Cerebellar syndromes; Dysdiadochokinesia; Parkinsonism; Rebound phenomenon; Saccades Dysmorphopsia the term dysmorphopsia has been proposed for impaired vision for shapes, a visual recognition defect in which visual acuity, colour vision, tactile recogni tion, and visually guided reaching movements are intact. These phenomena have been associated with bilateral lateral occipital cortical damage. Dysphagia of neurological origin may be due to pathology occurring anywhere from cerebral cortex to muscle. Neurological control of swallowing is bilaterally represented and so unilateral upper motor neurone lesions may cause only transient problems. Poststroke dysphagia is common, but there is evidence of cortical reorganization (neuro plasticity) underpinning recovery. Dysphagia of neurological origin may be accompanied by dysphonia, palatal droop, and depressed or exaggerated gag reex. Cross References Aphasia Dysphonia Dysphonia is a disorder of the volume, pitch, or quality of the voice resulting from dysfunction of the larynx, i. Hence this is a motor speech disorder and could be considered as a dysarthria if of neurological origin. Flaccid dysphonia, due to superior laryngeal nerve or vagus nerve (recurrent laryngeal nerve) palsy, bulbar palsy. Cross References Aphonia; Bulbar palsy; Diplophonia; Dysarthria; Dystonia; Hypophonia; Vocal tremor, Voice tremor Dyspraxia Dyspraxia is difficulty or impairment in the performance of a voluntary motor act despite an intact motor system and level of consciousness.
Article 116 stipulates that skin care nz buy cheap elimite 30 gm on line, in fulfilling its tasks acne zip back jeans cheap elimite 30gm on-line, the Confederation shall take due account of the needs of the family and may legislate on family allowances; this article provides the legal basis for maternity insurance acne jacket buy elimite without prescription. Many non-governmental organisations are in part subsidised by the state and carry out specific tasks related to family policy skin care face buy elimite with mastercard. The division of responsibilities among political levels and the number of actors involved is acne keloidalis cheap elimite 30 gm visa, therefore acne facials discount elimite 30gm on-line, complex. For instance, each political level intervenes in early childhood education and care: for example, though most childcare services stem from the market, they are regulated and partially subsidized by the communes and/or the cantons. Finally, the federal level is also involved through a temporary programme, which subsidizes new childcare initiatives and the creation of additional places for pre-school children. The Swiss political system is a direct democracy: through referendums and initiatives, citizens may challenge any law passed by parliament and propose amendments to the federal constitution. In the case of an amendment proposed to the federal Constitution, referendum is mandatory. Maternity leave (Allocation de maternite) (responsibility of the Federal Department of Home Affairs, Federal Social Insurance Office) Length of leave (before and after birth) Sixteen weeks, starting on the day of delivery. Companies, which often take out private supplementary insurance for such cases, cover these expenses. However, these regulations generally provide more generous maternity benefits to their employees, i. A minority of cantonal employers grant four additional weeks for mothers who are breastfeeding, bringing their leave up to twenty weeks. A cantonal Loss of Earnings Compensation fund pays for the two additional weeks, which are not covered for by federal dispositions. Working mothers who receive less than this amount through the federal entitlement will be entitled to the difference through this cantonal insurance. However, the existence, length and payment of a Paternity leave depends on the parties involved and social partners through the establishment of individual agreements, standard employment contracts, collective employment contracts, or well established common practices (even if not written) in a company or a branch. Regarding payment during these days off, it is generally understood that time off for the birth of a child should be paid; this is, however, not mandatory. There is no representative survey on the number of days off granted to fathers on a national scale and if they are paid. However, there are some indications that the majority of collective 194 labour agreements grant a minimum of one day off (the day of birth), and that it is predominantly paid for at 100 per cent by employers. Several small-scale research studies show that, increasingly, private companies and public administrations grant employees five days of paid Paternity leave (with full earnings compensation). More rarely, companies grant two or three weeks of paid Paternity leave and sometimes allow employees to take one or two additional unpaid weeks. This leave is generally to be taken at the birth of the child, but sometimes a longer time frame is given. Other employment-related measures Adoption leave and pay There is no federal statutory entitlement. Some cantons have implemented gender neutral adoption allowances for working parents, available to only one of the adoptive parents; the cantons of Vaud and Geneva entitle adoptive parents to 14 and 16 weeks of pay, 197 respectively, at 80 per cent. Such cantonal allowances are provided only if one of the parents interrupts his/her employment. Time off for the care of dependants Parents are entitled to three days per illness episode in order to care for their sick child upon presentation of a medical certificate. When two persons share parental responsibilities, only one should benefit from this provision (parents should decide who benefits from the leave for sick children, depending on the solution which suit them best). This leave is understood as time granted for lone parents or working parents in order to organise prolonged childcare if that is needed. Salary payment is suggested by the Code of Obligations as parents have a legal obligation to care for their dependent children; although salary payment seems to be a common practice, it is not mandatory. Family responsibilities are defined as the education of children up to 15 years old and the charge of other family members or close members in need of care. Relationship between leave policy and early childhood education and care policy the maximum period of paid post-natal leave available in Switzerland is just over 3. Changes in policy since April 2012 (including proposals currently under discussion) A 2007 parliamentary initiative demanding the ratification of the Convention No. Unless an optional referendum is deposited (official th deadline is 7 April 2013), the Federal Council will ratify the convention. In March 2013, the Swiss electorate voted on a new Constitutional article on family policy, which focused on work and family life reconciliation; 54. Ballot results show clear divides between the German-speaking and the French and Italian-speaking cantons (all of the latter accepted the new article), as well as between urban and rural cantons. The federalist political system implies that any amendment to the Constitution must reach a double majority (electorate and cantons). The new article proposed to assign to cantons the responsibility of providing an appropriate offer of extra-familial and extra-school childcare structures. The Federal Council (federal government) has also been systematically opposed to the introduction of Parental leave policies. It has, however, agreed (September 2011) to produce a report which evaluates the feasibility and costs of the different proposals, among others a tax-deductible private Parental leave insurance. Two parliamentary proposals must still be processed or were submitted since April 2012. One proposes to enable fathers (only those serving in the army) to transform their military service benefits into paternity benefits in the year of birth of the child or the year after. Finally, a Motion requests that Maternity leave be extended to adoptive parents of children under four years. The adoption leave would be financed through the Loss of Earnings Compensation Act (as for maternity benefits), but both mothers and fathers would be eligible. In May 2012, the Federal Council gave a negative recommendation to the Motion, arguing that adoption leave is closer to Parental leave than a Maternity leave and should be evaluated in the frame of the report on Parental leave policies to be produced by the Federal Department of Home Affairs. Maternity leave Approximately 70 per cent of women giving birth meet the eligibility criteria of maternity allowances and benefit from them. It is estimated that the majority of recipients take up the 199 maximum length of paid leave (98 days). The number of recipients has been increasing since Maternity leave was introduced, probably because of an increase both in births and female employment. According to Sottas and Millioud (2008), in 2006 80 per cent of leave recipients were married, 15 per cent single and five per cent divorced. The majority of recipients were employees (83 per cent); 14 per cent were self-employed and three per cent inactive (eligible because they previously received unemployment, health or disability benefits). For this reason, the average length of leave is under-estimated because some recipients receive part of their allowances on one year and the rest on another. There is some research on special Paternity and Parental leave entitlements available in public administrations and on common practices and/or needs in the private sector. Here again, research literature is either not totally up to date (the most recent data for cantonal entitlements for civil servants are 2008), partial (surveys on reconciliation measures in private companies concern only specific cantons), or non-existent. For instance, to my knowledge, there exists no overall view of collective agreements or standard work contracts that grant paid Paternity leaves or unpaid Parental leaves to employees. No representative statistics are available either on the proportion of working men and women who can benefit from such policies and who take advantage of them. Information about instruments and legal frameworks, covering a wide range of leaves and flexible working arrangements, are available and updated annually. It is based on a telephone survey of 402 companies and 335 women who had children in the last five years. Women working in the French and Italian regions are more likely to benefit from more generous schemes than employees in the German-speaking part. The study also reveals that the savings that companies make through the introduction of a maternity insurance are only rarely reinvested for Parental leave policies: 23 per cent use this money for more generous Maternity leave schemes; 20 per cent to replace the employee on leave; six per cent for a Paternity leave and 4 per cent for childcare services. Isabel Valarino, doctoral thesis at the Institute of Social Sciences, University of Lausanne. This research analyses the emergence and problematisation of Parental and Paternity leaves in the Swiss political and media spheres, as well as in work organisations. A case study in a public work organisation granting discretionary leave benefits and interviews with fathers benefiting from such policies will be conducted. Maternity leave (responsibility of the Department for Business, Innovation and Skills) Length of leave (before and after birth) Fifty-two weeks. A woman can start to take her leave from 11 weeks before the beginning of the week the baby is due. Medium and large employers can claim back 92per cent from the Exchequer and small employers can claim back 103 per cent. Flexibility in use the mother can opt to start her leave at any point from 11 weeks before the beginning of the week the baby is due until the baby is born. Women who have recently left work, changed jobs, or are self-employed may be eligible for this payment. To qualify, they must have worked for 26 weeks out of the 66 preceding the expected week of childbirth and have earned at least 30 per week on 13 of these weeks. They must have worked continuously for their employer for 26 weeks by the end of the fifteenth week before the start of the week the baby is due and remain employed into the week before the leave is due to start. If they do not, and the employer cannot accommodate the change, the father will have to take the leave on the dates he originally told his employer. For example, in 2007, 53 per cent of workplaces with five or more employees offered extra-statutory Maternity leave and 16 per cent provided additional 204 payments (Hayward et al. Paternity leave (responsibility of the Department for Business, Innovation and Skills) Length of leave Two weeks. Parental leave (responsibility of the Department for Business, Innovation and Skills) Length of leave Eighteen weeks per parent per child. Parents of a disabled child may take this leave up until the child is 18 years old. Flexibility in use Leave may be taken in blocks or in multiples of one week, (unless the child is disabled. Other employment-related measures Adoption leave and pay 205 Department of Trade and Industry, Parental leave, summary guidance. There is also a right to paid Paternity leave for an adopter not taking adoption leave (if they meet the eligibility criteria). Flexible working: the right to request and the duty to consider Employees who have parental responsibility for a child aged 16 and under, a disabled child under 18 years or who care for a spouse, partner, civil partner, relative or other adult living with them have a legal right to apply to their employers to work flexibly. Employees need to have worked for their employer continuously for 26 weeks before applying. Changes in policy since April 2012 (including proposals currently under discussion) Over the last year lobby groups (business, parent and child welfare organisations) have continued to debate leave and flexible working in response to the Consultation on Modern 208 Workplaces: flexible parental leave, flexible working, annual leave and equal pay proposed by the new coalition Government after it was elected in 2010. The Bill completed its committee stage on 25 April 2013, after a second reading debate on 25 February 2013. The Bill is wide-ranging, covering many areas beyond Shared Parental leave and flexible working. These earlier 211 proposals were to reduce the length of Maternity leave (currently 52 weeks) and pay (currently 39 weeks, mostly at a low flat rate) to 18 weeks; and to reclassify the remainder of existing Maternity Leave as Parental Leave. Proposals for the new Parental leave included: four weeks of paid Parental leave exclusive to each parent to be taken in the first year. By contrast, the Children and Families Bill introduced in February 2013 included the following proposals: Retention of Maternity leave duration to 52 weeks and Paternity leave duration to two weeks. This leave would be termed Shared Parental Leave (it is replacing a similarly designed 208 Department for Business, Innovation and Skills (2011) Modern Workplaces.
Purchase elimite 30 gm otc. How To Get Clear Skin In 3 Days | Skin Care Regimen.
References
- Gross MS, Broghammer JA, Kaufman MR, et al: Urethral stricture outcomes after artificial urinary sphincter cuff erosion: results from a multicenter retrospective analysis, Urology 104:198n203, 2017.
- Clark D. 'Total pain', disciplinary power, and the body in the work of Cicely Saunders, 1958-1967.
- Arborelius L, Owens MJ, Plotsky PM, Nemeroff CB. The role of corticotropin-releasing factor in depression and anxiety disorders. J Endocrinol 1999;160(1):1-12.
- Goldmuntz E, Clark BJ, Mitchell LE, et al. Frequency of 22q11 deletions in patients with conotruncal defects. J Am Coll Cardiol. 1998;32:492-98.
- Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009;338:1665.
- Nanda S, Nelson-Piercy C, Mackillop L. Cardiac disease in pregnancy. Clin Med. 2012;12(6):553-60.
- Johnson LH, Bhutani VK, Brown AK. System-based approach to management of neonatal jaundice and prevention of kernicterus. J Pediatr 2002; 140: 396-403.
- Koh EJ, Wang KC, Phi JH, et al. Clinical outcome of pediatric choroid plexus tumors; retrospective analysis from a single institute. Childs Nerv Syst 2014; 30(2):217-25.