
David A D'Alessio, MD
- Professor of Medicine
- Chief, Division of Endocrinology and Metabolism
- Member of Duke Molecular Physiology Institute

https://medicine.duke.edu/faculty/david-dalessio-md
It can arise from previously normal skin or from a pre-existing lesion (such as Bowens disease and actinic keratosis) heart attack connie talbot generic diovan 80 mg without a prescription. Common sites include bald scalp blood pressure chart 60 year old buy diovan cheap, lower lip arrhythmia in newborns order 160 mg diovan free shipping, cheeks blood pressure normal lying down diovan 80 mg discount, nose heart attack remixes 20 80mg diovan with amex, top of ear lobes and dorsum of the hand arteriosclerotic heart disease order generic diovan online. They can also appear on non sun-exposed sites such as a site of previous radiotherapy or chronic scarring of burns and leg ulcers. If the lesion is superfcial (that is, it has not invaded downwards into the dermis), excision is more likely to result in cure. Change or irregular colour Malignant melanoma Minor features (score 1 point) A malignant melanoma is a malignant tumour of the pigment-producing 1 point. Oozing or bleeding of the skin cancers as it has the capability to metastisise through the 1 point. Suspect melamona if any major feature is present or there is a total score Approximate age group of 2. All age groups, particularly in those with fair or red hair who burn rather than tan in the sun. If urinalysis identifes protein or blood in the urine, specialist help should be sought as the patient may require systemic steroids or cyclophosphamide. Where no cause can be found (idiopathic), the patient should be reassured that the condition is self limiting and should resolve within 36 weeks. Vasculitis Advice to patient Vasculitis is an infammation of the blood vessels in the skin, usually due Bed rest will stop new lesions forming. Regular analgesia should be to the deposit of immune complexes in the walls of the vessels. Henoch-Schonlein purpura is a form of vasculitis and occurs mainly in the young (see section 05). Presentation the presentation will differ depending on the size and site of vessels involved. If the capillaries are involved, there will be a polymorphic rash with palpable purpura, as well as macules, papules, vesicles and pustules. If there is arterial involvement, livedo reticularis, nodules and ulceration of the lower leg may be present. Where there is arterial and venous involvement, there will be red, tender nodules or deep plaques in the subcutaneous fat. The patient may be feverish before developing a rash which will start with pink macules. The condition is communicable from fve days before the rash develops until around six days after. The spots can be very itchy and secondary infection may lead to pock-like scarring. However, an antiseptic-based emollient may reduce the risk of secondary infection. In adults or immunocompromised patients, aciclovir, valaciclovir or famciclovir will reduce the severity of the attack. Traffc light Adults who contract chickenpox can become very unwell with more severe symptoms. Chickenpox (Varicella) Varicella zoster virus causes chickenpox and shingles (see section 04 for shingles). By the age of 10 years most children, particularly in urban communities, will have been infected. Primary infection confers long-term immunity but the virus remains dormant in the dorsal root ganglion to be reactivated as shingles. Local dermatology nurses and dermatology departments will help with education, support and long-term management. The National Eczema Society, British Association of Dermatologists and the Primary Care Dermatology Society can also provide useful written Eczema (atopic) information. Atopy means an inherited predisposition to eczema, asthma or hay fever Traffc light and atopic individuals may have one or all of these conditions. The condition tends to be long term, but it will clear by puberty in 90% of individuals. Presentation In an acute reaction, the skin displays the signs of infammation: heat, erythema and swelling. Treatment If it follows a streptococcal infection, treat with phenoxymethyl penicillin. Proteinuria and microscopic haematuria without impaired renal function will normally get better spontaneously in less than four weeks. If acute nephritis or progressive renal failure occurs, the patient should be referred to a renal physician. Henoch-Schonlein purpura this is a form of vasculitis (infammation of the small blood vessels) in the skin and various other tissues in the body. Three-quarters of cases are preceded by an upper respiratory tract infection, mostly caused by haemolytic streptococci. Several other associations have been reported including drugs, food and various infections. Approximate age group Mainly seen in children under the age of 10 years, with a slight male predominance. Once the crust has been removed, apply the topical treatment to the affected area, ensuring that the treatment is applied to the nares at the same time. If the patient has widespread lesions or impetiginised eczema, systemic antibiotics, such as fucloxacillin or erythromycin if allergic to penicillin, are advised. Advice to parent/carer Encourage good basic hygiene practices to limit contact and spread of the condition: this includes advice to avoid sharing towels and facecloths Impetigo and encouraging good handwashing technique after contact. As A superfcial infection of the epidermis caused by Staphlococcus aureus, scratching may spread the lesions, keeping the nails short is advisable. The condition is Impetigo can occur as a secondary infection in excoriated skin such highly contagious. Presentation Typically starts as vesicles which rapidly break down to form honey- coloured crusts; less commonly, there may be just a glazed erythema. Sites usually involved are the face and neck but it can spread extensively over the body. If the lesions are widespread, treat with oral anti staphylococcal antibiotics such as fucloxacillin or clarithromycin. Impetiginised eczema Secondary infection, most commonly with Staphlococcus aureus or streptococcal isolates, can occur in the broken skin caused by scratching in atopic eczema. Presentation It is important to establish if the patient has a history of atopic eczema. The skin may be weeping with papules and crusts and be rapidly worsening despite using standard treatment for eczema. Miliaria rubra (prickly heat) occurs deeper in the epidermis and results in itchy red plaques. Miliaria profunda results from sweat leaking into the dermis causing deep, intense, uncomfortable, prickling red lumps. Presentation Typically, folliculitis develops in the skin folds and on the body, especially in areas of friction from clothing. In infants, lesions commonly appear on the neck, groins and axillae but can also appear on the face and elsewhere. In contrast to acne and other forms of folliculitis, miliaria spots do not arise around hair follicles. Koplik spots on the buccal mucosa are diagnostic at this stage (these look like grains of salt on a red base). Around day 4, a red macular rash will appear behind the ears and spread to the face, trunk and limbs. Bed rest is advisable if the child is sick and pyrexia can be treated with paracetamol elixir. A barrier moisturiser such as zinc and castor oil cream should then be applied to the area covered by the nappy. Disposable nappies are more suitable than towelling ones while skin is affected as they are more effective at drawing liquid away from the skin. Napkin dermatitis (nappy rash) the common type of nappy rash is an irritant contact dermatitis, caused by urine and faeces being held next to the skin under occlusion. Bacteria in the faeces break down the urea in the urine into ammonia which irritates the skin. Presentation the rash will be patchy and tends to involve the skin in contact with the nappy (buttocks, genitalia, thighs); the skin folds may be spared. Only erythema is present in mild cases, but erosion or even ulceration can occur in severe cases. Rubella (German measles) Rubella, caused by a rubivirus, is a common viral illness in children. Presentation After an incubation period of 1421 days, a macular rash begins on the face and neck. It spreads down the body in 2448 hours then clears from the face downwards in 23 days. It is associated with enlarged occipital and posterior cervical lymph nodes and, occasionally, an arthritis. If itch keeps the patient awake at night, a sedating night-time antihistamine can be prescribed. Advice to patient If there is a family pet (cat or dog) and fea bites are suspected, the animal, rather than the human, should be treated. Bites (insect) the presentation of the bite will help determine the causative insect. If there are groups or rows of 3 or 4, think of fea bites; bed bug bites produce single very large lesions on the hands or face, with new lesions usually being found each morning. Numerous other insects can bite humans, including midges, mosquitoes, fies, wasps, tics, bees, ants, moths and butterfies, centipedes, ladybirds and spiders. Treat adults with a 7-day course of an oral antiviral agent such as aciclovir, valaciclovir or famciclovir. In children, topical aciclovir can be prescribed if infection is mild, and oral aciclovir if severe. These drugs are only effective when the virus is replicating so should only be given in the early phase of the disease (within 48 hours of the rash appearing). Adequate analgesia, such as paracetamol or co-dydramol (adults only), is important. Advice to patient/parent Good hygiene: avoiding the sharing of towels and good handwashing techniques are important to minimise the risk of spreading the infection to others. Traffc light In children, hospitalisation may be considered in cases of severe infection. Presentation the rash is made up of small umbilicated vesicles or grouped punched- out erosions which are painful rather than itchy. The patient will be generally unwell, which you would not normally expect with atopic eczema. Uraemia (also seen in 80% of patients on maintenance haemodialysis) Check creatinine and urea. Obstructive jaundice (may occur in patients with primary biliary cirrhosis before jaundice occurs) Check liver function tests and autoimmune profle. Thyroid disease Both hypo- and hyperthyroidism: check T4 and thyroid stimulating hormone levels. Lymphoma Especially in young adults, check for enlarged lymph nodes clinically and on chest x-ray. Psychological Presentation Look for evidence of depression, anxiety or emotional upset. In generalised pruritus, the patient presents with itchy skin all over with no visible rash but may have evidence of excoriation due to scratching. A detailed history is required as there are many possible causes of pruritus, which include the following. If the itch is not settling and is interfering with sleep, a sedative antihistamine should be prescribed to be taken an hour before going to bed. Traffc light the patient often feels dirty and may describe a feeling of something crawling under the skin. Encourage frequent use of emollients and encourage patting (not rubbing) skin dry after bathing. Traffc light A frequent accompanying feature of urticaria is angioedema, in which oedema develops in the subcutaneous tissues around the eyes, lips, mouth and in the pharynx. If life-threatening swelling of the larynx or tongue occurs (anaphylaxis), follow local guidelines. Urticaria (acute) Urticaria refers to a group of disorders caused by the release of chemicals such as histamine from the mast cells in the skin. Presentation the skin itches or stings, with the development of weals which are frst white, then turn red.
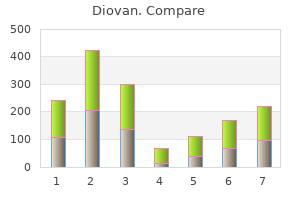
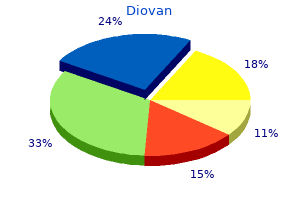
For people with epilepsy prehypertension at 24 buy diovan 40 mg cheap, prescribing issues centre on consistency of supply rather than favouring a branded product over a generic product blood pressure chart teenager buy diovan 160 mg lowest price. A major focus at Epilepsy Society is to investigate and understand the genetic architecture underlying the many causes of epilepsy blood pressure cuff cvs proven diovan 160 mg. Epilepsy charities have been campaigning for of epilepsy and tackle some of the misconceptions and stigma around epilepsy blood pressure chart low buy 160mg diovan. Our Everyone knows stronger warnings about risks associated with the drug and the effect on the unborn child hypertension teaching order diovan 80mg on-line. Making people more epilepsy aware is key to Epilepsy Societys training programme blood pressure normal low pulse rate purchase 40mg diovan free shipping. The toolkit explains the potential risks for an unborn child exposed to the drug during pregnancy. This would provide the necessary information to tackle premature mortality in epilepsy. Epilepsy Society has also been working with the Ministry for Transport to improve accessibility on public transport for people with hidden disabilities. Epilepsy Societys helpline is accredited by the Telephone Helpline Association for the quality of the service it provides. Many of the calls they receive begin as a seemingly straightforward request for information, and then develop into a more intense conversation in which the caller begins to explore areas of deeper concern. Young Epilepsy offers a helpline service and Epilepsy Actions helpline is a freephone number. We support hospital volunteers across the country through provision of free information of issues that impact on those affected by epilepsy. This includes material about employment, pregnancy, benefits, driving and medications. Raising awareness Understanding and raising awareness of epilepsy among the general population and reducing stigma around the condition is key to improving the lives of people with epilepsy. The voluntary organisations have an important role to play, informing and educating. Epilepsy can often be an isolating condition, but social media is helping bring people together. Epilepsy Society now has almost 50,000 followers on Facebook and 18,600 on Twitter. This gives us an average monthly reach of 500,000 people on Facebook and 200,000 on Twitter. A social media campaign around people being mistaken for being drunk during or after a seizure, reached 200,000 people on line with additional national media online viewers totalling more than 15 million. The British Association of Social Workers states: Social work practice addresses the barriers, inequities and injustices that exist in society. It responds to crises and emergencies as well as to everyday personal and social problems. Social work utilises a variety of skills, techniques, and activities consistent with its holistic focus on persons and their environments. Social work interventions range from primarily person-focused psychosocial processes to involvement in social policy, planning and development. These include counselling, clinical social work, group work, social pedagogical work, and family treatment and therapy as well as efforts to help people obtain services and resources in the community. Interventions also include agency administration, community organisation and engaging in social and political action to impact social policy and economic development. The holistic focus of social work is universal, but the priorities of social work practice will vary from country to country and from time to time depending on cultural, historical, legal and socio-economic conditions. These include: Medical model A medical practitioner may view a physical disability as a dysfunction or abnormality located within an individuals body. Within medicine there are different ways of categorising disability: in terms of specific medical diagnosis; the bodily system affected; functional loss. However, when looking at the nature and variability of impairments it becomes clear that for some conditions the degree of physical impairment cannot be predicted by the medical diagnosis as the physical consequences vary from person to person. The experience of the impairment also varies within the same person, as impairment is rarely fixed. Historically, disabled people came to be perceived as sick and as in need of a cure. Traditionally the role has been to assist the disabled person to adjust to their impairment. Therapeutic work based on behavioural or cognitive perspectives may focus on improving coping strategies. Social model In contrast to the medical and some psychological models, in 1983 the disabled academic Mike Oliver coined the phrase social model of disability. The social model of disability is based on a distinction between the terms impairment providing welfare systems on the basis of individual need has aided the process of excluding disabled and disability. Disability is used to refer to the restrictions caused by society when it does not give equivalent People with disabilities, including epilepsy, can face infantilisation. Disabled people can find themselves in a socially devalued and disempowered position. The needs-led assessment should address a range did not intend the social model of disability to be an all-encompassing theory of disability, rather of activities geared towards reducing risk, maximising independence and improving quality of life. With his theory, if a building has ramps and Support services for people with epilepsy should include the promotion of employment, education and slopes it would be accessible for wheelchair users. Within the inclusive environment the wheelchair leisure opportunities as part of a programme of developing independence and life skills. Disability and management of risk of harm A holistic approach looks at the whole of the clients life rather than just their body, psyche or social the Report of the Inspection of Scottish Borders Council Social Work Services for People Affected environment to maximise their independence and improve their lifestyle. As with other socially by Learning Disabilities outlines substantial failings in services designed to protect vulnerable adults. They may need assistance in gaining access to and a learning disability over a lengthy period. Promoting to society a more positive attitude toward epilepsy so that others do not themselves. The report also implied that disablement factors may discriminate against a person underestimate the potential quality of life of those who experience seizures. Unfortunately there are areas of the service provision where the persons need for care, support and protection in the community is not met. For example, a social worker could and the risk to the person of failing to meet those needs. A referral could be made to an occupational therapist for an assessment A social worker working with service users with epilepsy has to look at all aspects of that persons of the clients property for adaptations. Sexuality is included in psychological measures of quality of life, such as the World Health service to remind a person to take anti-epileptic medication, or equipment such as a one-cup Organizations Quality of Life Scale. However, sexuality is often omitted from the representations of water dispenser to reduce the risk of scalds in the kitchen. To start later if a person has a seizure in the night or early morning, or provide and that this is fuelled by the belief that disabled people are incapable of having or being interested a screen for privacy if a person has a seizure at work, and a quiet space to recover. A social worker can learn Berman et al11 examined sexual knowledge, sexual behaviour and beliefs about sexuality among from the service user the physical consequences relating to their impairment, as well as the emotional adolescents with congenital physical impairments. The authors felt that the lack of research in this and cognitive experiences and the constraints of living in an able-bodied biased society/environment. They found Social work with disabled client groups that adolescents with physical impairments are generally uninformed or misinformed about sex and sexuality and how these relate to their impairment. Disabled people are a recognised group of people who face discrimination and oppression. It is important to move away from a medical model where the emphasis can be agencies which help a person find a partner, while providing support and assessing risk. A social worker to focus too much on care and doing things for people and not enough on rights and empowerment. The fact remains for an able-bodied person becoming a publicly controlled experience for a person with epilepsy. The model looks at the underestimation of the potential includes personal dignity, being treated with respect, and control by the individual over their day-to-day of disabled people to add economic value to society if they are given equal rights and equally suitable life. The Act requires that attention is given to the individuals views, wishes, feelings and beliefs. Personalisation the report also found that disabled people were unwilling to enter the labour market because the the Care Act 2014 promotes personalisation and outlines scope for individuals who have eligible consequent reduction in their disability benefits would make it not worthwhile to undertake employment. Personalisation is a social care approach described by the Department people back into work; and tackling discrimination in the workplace via anti-discrimination policy. But the requirement of employers and service providers to make personal budgets, under which they can choose the services that they receive. Personalisation should reasonable adjustments to their policies or practices and physical aspects of their premises follows also mean that those services are tailored to the needs of every individual rather than delivered in the social model. By making adjustments, employers and service providers are removing the barriers a one-size-fits-all fashion. It should also allow better provision of improved information and advice that disable. The Equality Act 2010 makes it unlawful for employers to ask questions about a persons epilepsy at a job interview or for a referee to comment on such in a reference, except where there Appendix: Legislation and guidance to be replaced in whole or part is a need to make reasonable adjustments for an interview to proceed. The following summarises some of the key legal provisions and existing statutory guidance which are to be replaced by the Care Act 2014 and the associated regulations and guidance. A social worker will be able to support a person with epilepsy in seeking either paid employment or voluntary work, advising them of their rights and signposting them to organisations such as the Shaw Where existing provisions relate to jurisdictions other than England, the provisions will be disapplied Trust (a not-for-profit organisation which helps disabled people find and sustain employment or enjoy so that they no longer relate to English local authorities. Where provisions relate to children as well more independent living) or the Disability Employment Advisor (within the Job Centre Plus). The repeals and revocations required will be provided for by Orders under the Care Act. The Care Act 2014 the final detail of which precise provisions are to be replaced is to be confirmed during the consultation In the past, obtaining support from community social services has been a postcode lottery. The areas listed below are not therefore a final position, but are intended to give an indication Act 2014 modernises and consolidates the law on adult care in England into one statute and has been of the scope of the Act and the key existing provisions which are to be affected. Report of the Inspection of Scottish Borders Council Social Work Services for People Affected by Learning Disabilities. Disability and the transition to adulthood: Issues for the disabled child, the family, and the paediatrician. Sexuality and the adolescent with a physical disability: Understandings and misunderstandings. The epilepsy lecture notes are the most comprehensive and up to date guide to managing epilepsy in the 21st century, and are invaluable to clinicians from primary to tertiary care. Although only compounded electrical potentials can be recorded on the surface electrophysiology is one of the fundamental diagnostic tools for the neurologist. Other electrophysiologic diagnostic tools like evoked potentials followed thereafter. Only the electrical currents in the radially oriented apical dentrites of the neocortical pyramidal neurons can be sampled. The electrodes are named by their location (F=frontal, P=parietal, O=occipital, T=temporal, C=central) and an associated number. Odd numbers are assigned to the left hemisphere, even numbers are assigned to the right hemisphere (Hughes 1994). Low frequency (high pass) and high frequency (low pass) filters are then applied to exclude frequencies outside the range of interest. Referential montages involve the difference between an active electrode on the scalp and an inactive electrode, for example, an electrode on the ear or chin. Bipolar montages record the voltage difference between two active scalp electrodes. In referential recording an abnormality is localized by identifying in which channels the abnormalities is of highest amplitude. In bipolar recording a phase reversal of an abnormal signal indicate the localization of the origin of an abnormality (Hughes 1994). By convention signals with an upward deflection are considered negative and signals with a downward deflection are considered positive. Digital recording requires a sufficient sampling rate of the signal (at least twice the frequency of the desired signal) to avoid aliasing (=distortion) of the signal. Impedance checks of all electrodes are indispensible in digital and analog recording in order not to contaminate physiologic signal by environmental noise.
Order diovan without prescription. How to Improve Blood Circulation with Alternative Medicine.
Microsomal enzyme induction from long- term phenytoin administration may increase metabolism of 25-hydroxycalciferol prehypertension hypertension buy diovan 160 mg online, worsening the osteomalacia of uremia (59) blood pressure medication make you cough generic diovan 80 mg on-line. Although phenytoin accumulation may accompany studies have not demonstrated enhanced microsomal enzyme severe liver disease blood pressure during heart attack buy generic diovan 160 mg online, nonlinear kinetics and difficulty in esti- activity (49 heart attack low vs diamond order 40 mg diovan fast delivery,50) nhanes prehypertension purchase discount diovan online. Because 95% of a phenytoin dose is biotrans- mating hepatic metabolic capacity limit the clinicians ability formed heart attack jarren benton lyrics buy diovan 80mg low price, little parent drug accumulates, even in severe renal to predict dose adjustments. Nevertheless, accumulation of the glucuronide minations and gradual dose regulation are necessary. Some studies suggest that it Phenobarbital may inhibit phenytoin biotransformation (52), whereas others report no such effect (27,53). Phenobarbital (5-ethyl-5-phenylbarbituric acid) is a weak acid Dialysis affects phenytoin primarily by altering protein with a pKa of 7. This apparent contradiction may result from fluctuations anisms, whereas the remainder is metabolized by the hepatic in the free fraction of phenytoin during and after hemodialy- mixed-function oxidase system. Martin parahydroxyphenobarbital and N-hydroxyphenobarbital, are and colleagues (55) reported that only 2% to 4% of intra- inactive and are excreted by the kidneys. Phenobarbital is a venous phenytoin appeared in the dialysate of seven uremic potent inducer of the microsomal enzyme system (40). Effects of Renal Disease Finally, certain assays may give incorrect results in renally Although the half-life of phenobarbital has been reported to be impaired patients. The enzyme-multiplied immunoassay may unchanged in uremic patients (38), some accumulation should falsely elevate total plasma phenytoin levels in patients with be expected, as elimination of long-acting barbiturates depends severe renal insufficiency (56), tripling values obtained by more on renal excretion than on biotransformation. In impaired renal function, severe central nervous system useful method in patients with advanced renal disease (57). Effects of Liver Disease Plasma from patients with hepatic insufficiency also has Effects of Liver Disease reduced binding capacity for phenytoin (28,44,45). The degree Because a significant amount is excreted unchanged by the of impairment correlates with levels of serum albumin (18,58) kidneys, phenobarbital has been promoted as a useful agent in or total bilirubin (53), or both (29,44). Nevertheless, some studies have that the total number of binding sites is reduced as a result of found a prolonged half-life in certain hepatic illnesses. Animal lower albumin concentration in competition with bilirubin models with carbon tetrachloride-induced liver damage Chapter 47: Treatment of Epilepsy in the Setting of Renal and Liver Disease 581 showed a slight reduction in plasma clearance (60). In cir- necessary and can best be established by measuring levels of rhotic patients, phenobarbital half-life was prolonged com- primidone, phenobarbital, and phenylethylmalonamide. However, in Valproic Acid patients with acute viral hepatitis, no statistically significant prolongation of half-life or change in metabolic excretion Valproic acid (2-propylpentanoic acid) is a carboxylic acid clearly occurred, although only one dose of phenobarbital was with a pKa of 4. In a previous study, two cirrhotic patients with a resultant volume of distribution of only 0. Elimination is mostly by hepatic biotransformation, with However, this study lacked controls and was complicated by only 1% to 3% of the dose excreted unchanged in urine. Biliary excre- than 70% is present as metabolites, primarily the glucuronide tion of phenobarbital is minimal, and cholestasis does not of 2-propylglutaric acid. Its metabolites show anticonvulsant activ- ity in animal studies, particularly 3-oxovalproic acid, which Clinical Recommendations has activity comparable to that of valproic acid in mice. No Although no short-term dosage adjustment appears necessary, data on this compounds activity in humans are available (65). The effect of liver disease on patients receiving pro- As with phenytoin, protein binding of valproic acid decreases longed phenobarbital therapy varies with the individual as in uremia (66,67). The decrease correlates with levels of blood well as with the type of liver damage. Frequent measurement urea nitrogen, creatinine, uric acid, and creatinine clearance of plasma concentrations will help establish dose modifica- but appears to have little relation to albumin and total protein tions; free levels offer little additional information. Hypoalbuminemia exerts a more significant effect in patients with a nephrotic syndrome than in healthy individ- uals. Hemodialysis decreased protein binding in 3 of 4 Primidone patients in one study (67). Reduced protein binding, with increased apparent volume of distribution, lowers total Primidone (2-deoxyphenobarbital), structurally related to steady-state concentrations and unchanged free levels. Approximately 20% of metabolites may have a prolonged effect because of delayed a primidone dose is excreted unchanged in the urine (9). A single case report of valproic acid-related hepa- tobiliary dysfunction and reversible renal failure described Effects of Renal Disease decreased renal clearance of total conjugated valproic acid. In Although little information is available on the use of primi- vivo production of rearranged valproic acid glucuronide was done in renal disease, accumulation with resultant toxicity has detected. It is unclear whether the accumulation of these been reported, presumably from delayed renal excretion and altered substances is related to hepatobiliary or renal dysfunc- prolongation of the phenylethylmalonamide half-life. In one tion, or both, and whether these substances are clinically report (63), phenylethylmalonamide levels were proportion- active in humans (69). Effects of Liver Disease Another patient showed evidence of intoxication, with high Valproic acid disposition studies in patients with alcoholic cir- phenylethylmalonamide levels and moderate elevation of phe- rhosis and those recovering from acute viral hepatitis (70) nobarbital in association with renal failure (64). Plasma half-life increased As primidone is metabolized to active compounds by the liver, from 12. Total drug plasma clearance remained unimpaired in lar to those seen with phenobarbital may be expected. No both groups, but free drug clearance decreased in cirrhotic results from experimental investigation of primidone in liver patients. The investigators noted Clinical Recommendations no changes in urinary excretion of valproic acid. Therefore, Because primidone is metabolized to three active compounds, liver diseases studied appeared to result in reduced metabolic determination of plasma concentrations may help in assessing capacity for valproic acid that was compensated for by intoxications. Although it is unclear whether primidone patients in acute stages of viral hepatitis showed increased may be removed by dialysis, its metabolite phenobarbital half-life of valproic acid from 14. A Hooper and associates (78) found no evidence of reduced pro- case resembling Reye syndrome in a 7-year-old reported sig- tein binding in patients with renal disease. Because only 1% of nificantly increased formation of three monounsaturated and carbamazepine is eliminated unchanged in urine, accumula- four double-unsaturated metabolites in plasma (58% to 71% tion of parent drug or the epoxide metabolite is unlikely. No of valproic acid compounds compared with a maximum of studies are available on the effects of dialysis on the drug or its 15% in controls) and in urine (34% to 61% compared with a metabolites. Serum-free carnitine, as well as the main - Significant reduction in the percentage of carbamazepine oxidation metabolite 3-ketovalproic acid, decreased despite bound to protein occurred in patients with mild liver disease serum valproic acid concentration at the upper limit of the (78). No clear correlation between any laboratory parameter therapeutic range in a 3-year-old with valproic acid-induced and the degree of impairment could be determined. Autopsy of a set of twins with a pro- gressive hepatic encephalopathy revealed hepatic necrosis Clinical Recommendations only in the sibling who had received valproic acid, indicating Dose adjustment is not needed in either renal disease or dialy- that the drug may have aggravated pre-existing hepatic sis. Other suggested associated risk factors for this condition include developmental delay and polytherapy. Ethosuximide Histologic changes are variable, including cholestasis, cen- trilobular necrosis, and fatty changes. Clinical symptoms, Ethosuximide (2-ethyl-2-methylsuccinimide), a weak acid such as nausea, vomiting, malaise, and breakthrough seizures, with a pK of 9. Accumulation in renal failure is unlikely Clinical Recommendations because of the small amount excreted. Significant removal Reduction of valproic acid dose generally is unnecessary in during dialysis is probable, owing to the low volume of distri- renal disease. However, decreased protein binding will lower bution and negligible protein binding. Supplementation based the therapeutic range in uremic patients in proportion to the on serum levels following dialysis is recommended (62). No estimated relationship has been established as it has for phenytoin, but free levels can be determined and dose adjustments should be based on clinical Benzodiazepines grounds and on the increase in free level greater than 10%. No clear evidence indicates that valproic acid must be sup- the most commonly used benzodiazepines in epilepsy are plemented following dialysis. Extreme caution should be diazepam, clonazepam, chlordiazepoxide, clorazepate, and exercised in the use of valproic acid in liver disease. All undergo primarily hepatic biotransformation; Significant accumulation may occur as a result of increased minimal amounts appear unchanged in urine. Various half-life and may worsen hepatic function to a precipitous metabolites such as desmethyldiazepam and oxazepam are degree. The literature has little information on such cases, as clinically active and eliminated by the kidney in the free and valproic acid was discontinued promptly in all reported glucuronidated forms. Levels of chlor- a neutral iminostilbene that is structurally related to diazepoxide and diazepam have not been found to decrease imipramine. The most signif- Effects of Liver Disease icant product is 10,11-carbamazepine epoxide, which has Liver disease significantly alters the disposition of most pharmacologic activity in animals (77). Prolonged half-life of diazepam and chlor- induce its own metabolism, shortening the half-life propor- diazepoxide has been found in cirrhosis and acute viral hepati- tionately to the duration of treatment (40). Notably, oxazepam shows no evidence of altered Chapter 47: Treatment of Epilepsy in the Setting of Renal and Liver Disease 583 disposition in various liver diseases (84,85). Maintenance dose reduction is appropriate for patients reduces protein binding in all benzodiazepines studied except with severe renal impairment, and close monitoring is war- oxazepam (86). For patients with hepatic impairment, the package insert recommends no dose adjustment for those with mild liver Clinical Recommendations disease, and a 25% reduction in initial, escalation, and mainte- Because renal disease has little impact on the elimination of nance doses in those with moderate liver disease or with severe benzodiazepines, no postdialysis supplementation or dose disease but no ascites. In the setting of severe liver impairment adjustment in uremia should be necessary. Oxazepam appears to be an exception, as it is eliminated after Felbamate glucuronidation without significant oxidative metabolism (8). Felbamate (2-phenyl-1,3-propanediol dicarbamate) is a dicar- bamate that is structurally similar to meprobamate. Plasma mate metabolites, none of which demonstrates significant protein binding is approximately 55% at therapeutic levels. Lamotrigine is metabolized predominantly by glucuronidation, and then it is eliminated renally. It may induce its own metabo- Effects of Renal Disease lism to a modest degree when multiple doses are administered Few data are available regarding the use of felbamate in (88). However, lamotrigine clearance is Effects of Liver Disease decreased by about 50% in the presence of valproate. As of September 1999, there were 19 reported cases of hepa- totoxicity associated with felbamate administration and 5 Effects of Renal Disease fatalities. The risk of fatal liver damage associated with felba- Clinical experience in patients with renal dysfunction is lim- mate is estimated to be 1 in 24,000 to 32,000 patients (92). In a study of a small number of patients with renal A detailed review of the reported cases of hepatic failure in impairment, Fillastre and colleagues (89) found that the elimi- patients treated with felbamate reveals confounding factors in nation half-life of unchanged lamotrigine is prolonged in com- up to 50% (93). Concomitant medications (valproic acid, car- parison with that in patients with normal renal function. Until further data are forthcoming, the clinician should hours in healthy volunteers. Approximately 20% of the consider potential risks for aplastic anemia and hepatic failure amount of lamotrigine present in the body was eliminated before initiating treatment with this drug. Clinical Recommendations Effects of Liver Disease Felbamate should not be prescribed for patients with a history the disposition of lamotrigine in patients with hepatic dys- of hepatic dysfunction. A patient who develops abnormal liver function has not been extensively evaluated. Posner and col- function values should be immediately withdrawn from the leagues (90) evaluated the pharmacokinetics of a single dose drug. Because felbamate is metabolized by the kidneys as well of lamotrigine in seven patients with Gilbert syndrome, a as the liver, either renal or hepatic dysfunction could decrease benign condition associated with a deficiency in the enzyme drug clearance. Because of the risk of aplastic anemia or bilirubin uridine diphosphate glucuronyltransferase. It does not bind to Lamotrigine should be used with caution in patients with renal plasma proteins and does not affect steady-state concentra- or hepatic dysfunction. Topiramate Effects of Liver Disease Topiramate, a sulfamate-substituted monosaccharide [2,3:4,5- Because of its low protein binding and renal elimination, bis-O-(1-methylethylidine)- -D-fructopyranose], is struc- gabapentin is theoretically a good anticonvulsant choice in turally distinct from other anticonvulsant drugs. However, currently few data are available regarding the use of Only 20% of a single dose is metabolized by healthy adults; gabapentin in this population. The drug is eliminated renally, and about 50% Gabapentin dosage should be decreased or the dosing interval to 80% appears unchanged in the urine (4). The manufacturer recommends the following dosages, based on the patients cre- Effects of Renal and Liver Disease atinine clearance: 400 mg three times a day, more than As topiramate is excreted primarily via the kidneys, impaired 60 mL/min; 300 mg twice a day, 30 to 60 mL/min; 300 mg creatinine clearance may delay elimination. In preclinical stud- once a day, 15 to 30 mL/min; and 300 mg every other day, less ies, topiramate was associated with a 1. A maintenance dose of 200 to 300 mg is rec- renal stone formation, but this rate was not greater than that ommended following each 4-hour session of hemodialysis, with seen in placebo-treated patients (101). No increased incidence no need for further supplementation until the next dialysis. Oxcarbazepine Clinical Recommendations Oxcarbazepine (10,11-dihydro-10-oxocarbamazepine) is the Topiramate has not been associated with hepatic disease. This compound was devel- Renal disease is not a contraindication to the use of topira- oped in an attempt to improve the tolerability profile of car- mate, although doses should be decreased and dosing inter- bamazepine by elimination of metabolic production of carba- vals lengthened in patients with impaired renal function. Oxcarbazepine is rapidly and Topiramate should be used with caution in patients with a his- almost completely absorbed from the gastrointestinal tract tory of probable kidney stones.
The etiologies of stroke in childhood are multitude blood pressure negative feedback loop buy discount diovan 40mg on-line, will remain an important area for investigation (6) blood pressure chart diagram buy diovan 40mg mastercard. Although relatively uncommon heart attack cafe menu 80 mg diovan with amex, the reported inci- seizures and subsequent epilepsy in children with stroke has dence has increased with better data collection blood pressure for heart attack generic diovan 160 mg fast delivery, improved been highly variable heart attack toni braxton babyface order diovan 40 mg without a prescription, partly based on few prospective studies blood pressure chart usa generic diovan 40 mg on-line, imaging modalities, and better recognition and awareness selection bias, small sample size, lack of long-term follow-up, amongst physicians. Data regarding seizure presentation and stroke patients from the prospective Canadian Ischemic Stroke subsequent epilepsy risk for hemorrhagic stroke in childhood Registry have shown an incidence of 6/100,000 children per is much less clear, with only few descriptive series. Similarly, in an times more commonly involved than the posterior circulation autopsy series of 592 infants (32), 5. Generalized and sub- followed 675 patients with a first stroke for a minimum of tle seizures, including apnea, and electrographic seizures 2 years, and found a 7. They found that the later onset seizures were overall mean from these studies would suggest a risk of about significantly more likely to recur (develop poststroke epilepsy) 22% for the subsequent development of epilepsy (22). In a retrospective study of stroke appears to predict the earlier onset of epilepsy in one Rochester Minnesota residents, 192 patients were identified recent large cohort (44). Abnormalities include Two key points were made by this study: the acute sympto- focal or generalized slowing; focal, multifocal or bilateral matic seizures had a much higher 30-day mortality (41. Periodic lateralized epileptiform discharges was 33% for the acute symptomatic seizure group and 71. Subcortical infarcts (basal ganglia, thalamus) have also been Early poststroke seizure: One or more seizures within the first associated with seizures either as an isolated presenting fea- week after the stroke. The semiology Late poststroke seizure: One unprovoked epileptic seizure at of the seizures is variable and often patients have more than least 1 week after the stroke. The occurrence of seizures and/or the prevalence of poststroke epilepsy has been reported altered level of consciousness at the initial presentation of variably from 2% to 4. The number of the patients is small, but quence of perinatal stroke dates back to the latter part of the these patients tend to have early onset status, nonconvulsive 19th century (48,49). The first detailed series of hemispherec- seizures with no apparent clinical signs, and increased mortality. Approximately one third of these occur as acute Histopathology of the resected specimens documented infarcts symptomatic or early onset seizures and are predicted to have a due to vascular ischemia/stroke as the etiology in a number of higher 30-day mortality and decreased incidence of seizure recur- his cases (50). The prevalence of poststroke epilepsy is 2% to 4% in patients with new onset strokes. Epidemiology the reported incidence of poststroke seizure and epilepsy has Pathophysiology varied in the literature from 3. Based on animal models, acute sympto- the Oxfordshire community stroke project prospectively matic seizures are thought to arise from the penumbra Chapter 30: Epilepsy in the Setting of Cerebrovascular Disease 373 surrounding the infarction (61). Occlusion of middle cerebral suggest an increased risk to develop late onset seizures. Other factors proposed to effect early seizures stroke, 17% were found to have epileptiform discharges or are deposits of hemosiderin-causing focal cerebral irritability, seizures (66). The pathogenesis of late dictor of epileptiform discharges and/or seizures on continuous seizures and poststroke epilepsy is even less clear. Another possible trig- or more were twice as likely to have electrographic seizures. Twenty-eight percent of the seizures were recorded area of the old stroke in patients with late seizures. The same changes were not seen in patients who developed recurrent seizures (poststroke epilepsy) suggesting that the effect was not due to seizure alone (60,63). Treatment the treatment of poststroke seizures and epilepsy has been controversial. Cortical location, stroke severity, and hemorrhagic benzodiazepines) were shown to worsen functional recovery stroke all were shown to be independent risk factors on multi- in animal models of stroke (69). In additional to localization to randomized controlled trials of treatment for patients with the cortex, an island of spared cortex, infarct with irregular poststroke seizures or epilepsy. The risk of seizure recurrence borders, temporal-parietal location, and posterior cerebral after an early seizure has been reported from 13% to 43%. Though no studies have been con- after the first seizure to a control group of stroke patients with- ducted in poststroke epilepsy patients per se, a study com- out seizures. Seizure control was similar among all three would later develop seizures, and none in the control group drugs, but tolerability favored lamotrigine and gabapentin. Poststroke epilepsy: Epidemiology, pathophysiology and neonate: maternal-placental-fetal considerations. A study of cerebral palsies of early life, based upon an cephalogram, and magnetic resonance imaging study. Infantile hemiplegia treated by removing one cerebral hemi- and cerebral blood flow velocity measurements. Poststroke epilepsy in the copenhagen stroke ischemic stroke in childhood: a long-term follow-up study. Seizures associated with stroke in child- seizures in cerebral vein and dural sinus thrombosis: risk factors and role of hood. Stroke in children: the coexistence of epilepsy after an ischaemic hemispheric stroke. In a few of the neurocutaneous syn- target of rapamycin) pathway that is critical to cell cycle regu- dromes, epilepsy is the most common presenting symptom. When the index case has an identified pathogenic ditions, we will touch upon important aspects of comorbid mutation, family members at risk could be screened by look- neuropsychiatric conditions, and other organ system involve- ing for that specific mutation. In a case with no identifiable ment that impact decision making for medical and surgical mutations, the family screening could begin by testing of the treatment of epilepsy. Clinical, radiographic, and pathologic biologic parents by means of a complete physical including a findings are presented in the pictorial atlas (Chapter 5). Early onset of epilepsy is one of the impor- 60% of the patients are the only family members affected, tant risk factors for continuing seizures and cognitive disabil- suggesting a new spontaneous mutation (5). It is also not known if and how multiple epilepto- in the eyes (retinal hamartoma), renal cysts and angiomyolipo- genic tubers interact with each other leading to an unpre- mas, hepatic cysts, and pulmonary lymphangiomyomatosis. Secondary bilateral synchrony ation, and the presence of cells that are transitional forms appeared in 35% of children with tuberous sclerosis after the between these two types. On unenhanced brain computed age of 2 years, especially during drowsiness and sleep (15,16). Between 26% and 58% of children with and infants with immature myelination, the tubers are hyper- tuberous sclerosis and infantile spasms have autism, com- intense to unmyelinated white matter on T1 sequences and pared with 13% of patients with infantile spasms who do not appear hypointense on T2-weighted images. There is evidence to sug- raphy seem to play an important role in the cognitive out- gest that cortical tuber count and location is associated with come. The persistence of epileptic foci in anterior and poste- increased risk of infantile spasms (22). There also appears to rior areas is thought to be important in the development of be a correlation between increased number of tubers, develop- autistic traits, such as severe disability in verbal and nonver- ment of early seizures and developmental delay. These are, in the order of common occurrence; thin Chapter 31: Epilepsy in the Setting of Neurocutaneous Syndromes 377 linear bands extending radially from the ventricular surface to contraindicated. Extra caution is required for monitoring pre- white matter lesions tend to be predominant in frontal lobes. However, two key rules for planning surgi- intermittent obstruction at the level of the foramen of Monro. The tubers often intermingle with white mat- reflecting hemorrhage or calcification. And lastly, lack of infantile spasms to corticotropin is similar to the response of long-term longitudinal postoperative outcome studies make children with cryptogenic infantile spasms; however, those family counseling before surgery imprecise as there is always a with tuberous sclerosis have a higher relapse rate. Neurologic manifestations include seizures, varying tigations, bilateral subdural and depth electrode implantation degrees of mental retardation, migraine-like headaches, inter- encompassing wide regions of brain bilaterally followed by a mittent or progressive stroke-like episodes with focal deficits focused search for the epileptogenic tuber(s) with staged resec- such as hemiparesis, hemiatrophy, aphasia, and hemianopsia tion(s) has been reported from one center (35). The intracranial lesion is review of literature published between 1960 and 2006, Jansen thought to be due to proliferation of leptomeningeal vessels in et al. Not surprisingly, authors decreased venous return (venous stasis), and consequent focal found these observational case series incomparable due to hypoxia leading to cellular death. This is seen radiographically extreme variability in the collection and reporting of data as gliosis, volume loss, and calcification. Bilateral brain lesions occur in patients were selected for epilepsy surgery based on other (not 15% of children. Bilateral hemispheric involvement increases studied in the paper) criteria(s), such as semiology, functional the risk of seizure. Hemiparesis is often discovered for the drome is also known as encephalotrigeminal angiomatosis or first time around the seizure clusters before it becomes an encephalofacial angiomatosis. It remains unclear if fixed hemi- 1879 by Sturge, who thought that the neurologic features of paresis is a stuttering progressive hemiparesis that occurs due the syndrome resulted from a nevoid condition of the brain to acute (seizures, stroke-like episodes) over chronic (hypoxia similar to that affecting the face. Fixed hemiparesis was the first to report a case with calcifications seen on skull contralateral to the facial angioma eventually occurs in 50% roentgenogram. Transient episodes of hemiplegia, not related to clin- caused by somatic mutation. Bilateral hemispheric involvement usually shows subtle or no abnormalities in young infants who are, at a later increased severity of mental retardation (41). Onset of epilepsy before 2 years of age increases the risk of mental retardation and refractory epilepsy. The size of vention or secondary prevention (after first stroke-like cutaneous angioma does not predict the size of intracranial episode), but its efficacy is controversial, and there have been angioma. Usually it is in the V1 distribu- prophylactic aspirin were found to have 65% fewer strokes tion with variable V2 and V3 involvement. Medical and surgical treat- found on the nape of neck above or below the hairline, upper ment of glaucoma includes beta-blockers, carbonic anhydrase trunk, or even the extremities, and hence may escape recogni- ophthalmic drops, and surgery. Even when facial angiomas are visual loss by aggressive glaucoma management has important bilateral, intracranial involvement tends to be unilateral or implications for future epilepsy surgery that likely involves dominant (asymmetric) on one side (21,41). Presence of vascular malformation in the distribution of V1 segment increases the probability of glaucoma. There may be associated vascular abnormality in the conjuctiva, sclera, retina, and choroid. There is reported spontaneous remission or controlled epilepsy in nearly increased incidence of retinal detachment secondary to hemor- half (40). In medically refractory patients, presurgical evaluation rhages from the choroidal hemangiomas. The timing that may not be readily apparent in a young infant without an of surgery is important. Seizures are usually daily, cata- strophic and fail to respond to medical treatment. Somatic ents is critical as the long-term outlook for neurocognitive mutation is postulated as the underlying genetic mechanism. Cutaneous lesions cal dysplasia, gyral fusion, pial glioneuronal hamartomas, cor- may be subtle to detect due to their skin-like color and velvety tical astrocytosis, and foci of microcalcification. The cutaneous lesions may differ somewhat 5% of individuals, a rate that is slightly higher than in the gen- in histology. The potential for malignant transformation cortical malformations, and mesial temporal sclerosis. Age of presentation varied from ter, we use the term epidermal nevus syndrome to encompass 4 days to over 20 years. Besides cutaneous manifestations, there is a wide spectrum of clinical presentation involving multiple organs and systems. Children with this disorder may Chapter 31: Epilepsy in the Setting of Neurocutaneous Syndromes 381 develop seizures (13. Sirolimus for angiomyolipoma in tuberous sclerosis complex or lymphangioleiomyomatosis. Efficacy of sirolimus in treating tuberous sclerosis and lymphangioleiomyomatosis. Morbidity associated with tuberous scle- Seizures and mental retardation are also seen in approxi- rosis: A population study. I: Seizures, pertussis which irregular, hypopigmented skin lesions along the embry- immunisation and handicap. The tuberous sclerosis syndrome: Clinical onal lines of dermatologic fusion are seen. Autopsy showed magnetic resonance imaging and electroencephalography in 34 children gray matter heterotopias and abnormal cortical lamination in with tuberous sclerosis. Tuberous sclerosis: Long-term follow-up and longi- a patient in one series indicative of abnormalities in neuronal tudinal electroencephalographic study. Learning disability and epilepsy in an epidemiological sample of individuals with tuberous sclerosis complex. Magnetic resonance imaging in neurocutaneous syn- typically measures greater than 5 cm. Subependymal giant cell tumors in tuberous patients usually present with seizures or increased intracranial sclerosis complex. The treatment of west syndrome: A patients are T1 shortening (increased signal) in temporal lobe cochrane review of the literature to December 2000. Usually there is lep- patients with tuberous sclerosis and localization-related epilepsy.
References
- Barrette S, Bernstein ML, Robison LL, et al. Incidence of neuroblastoma after a screening program. J Clin Oncol. 2007;25:4929-4932.
- Joo H, Naik V: Conventional tracheal tubes for intubation through the intubating laryngeal mask airway. Anesth Analg 101:1245, 2005.
- Druml W, Fischer M, Sertl S, et al. Fat elimination in acute renal failure: long-chain vs medium-chain triglycerides. Am J Clin Nutr. 1992;55:468-472.
- OiDonnell B, Puri P: Endoscopic correction of primary vesicoureteric reflux, Br J Urol 58(6):601n604, 1986.
- Katkhouda N, Mavor E, Achanta K, et al: Laparoscopic repair of chronic intrathoracic gastric volvulus. Surgery 128:784, 2000.
- Gandhi SK, Bromberg BI, Schuessler RB, et al. Characterization and surgical ablation of atrial flutter after classic Fontan repair in acute canine model. Ann Thorac Surg. 1996;61:1666-78.
- Schroten H, Roesler J, Breidenbach T, et al. Granulocyte and granulocyte-macrophage colony-stimulating factors for treatment of neutropenia in glycogen storage disease type Ib. J Pediatr 1991;119:748.
- Fonarow GC: Practical considerations of-blockade in the management of the postmyocardial infarction patient. Am Heart J 2005;149:984-993.