
Bernhard Meier, MD
- Professor and Chairman of Cardiology
- Swiss Cardiovascular Center Bern
- University Hospital
- Bern, Switzerland
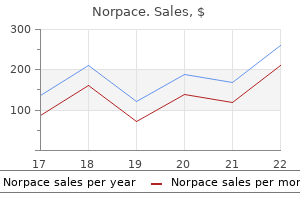
A resource for life Heart attack Heart damage from a blockage of a heart artery (also called a myocardial infarction) 84 Living with Kidney Disease: A comprehensive guide for coping with chronic kidney disease Hypertension High blood pressure treatment 3rd degree hemorrhoids discount 150mg norpace overnight delivery, which may be either the cause of medicine plies cheap norpace 150mg visa, or the result of medicine zantac buy discount norpace, kidney disease Im m unosuppressive Drugs that prevent or treat the rejection drugs of a transplant (also called antirejection drugs) Kidney biopsy Extraction medications zolpidem order norpace 100mg amex, using a needle medications made easy buy norpace 150 mg line, of a small piece of kidney tissue translational medicine safe 100mg norpace, which can then be examined under a microscope M em brane In the artifcial kidney, a porous material used to flter waste from the blood Nephritis See Glomerulonephritis Nephrology the branch of medical science that deals with the kidneys Nephron the structural and functional unit of the kidney, numbering over a million in each kidney. At high levels it causes itching and painful joints Phosphate binder A medication that binds with phosphate in the intestine, causing more phosphate to be passed in the faeces Polycystic kidney disease An inherited kidney disease that produces fuid-flled cysts in the kidneys that produce chronic kidney failure over many years Potassium A mineral in the body fuids that is regulated by the kidneys and, at normal levels, helps nerves, muscles and other cells work well. Am J Kid Dis 2009; 54(5): 798-809 Gotch et al, Effective diffusion volume fow rates (Qe) for urea, creatinine, and inorganic phosphorus (Qeu, Qecr, QeiP) during hemodialysis. Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. To-date, most patients using the System One are treating more than thrice weekly Due to increased frequency of therapy, potassium fuctuations are typically less extreme As a result, the amount of potassium added or removed per session is also smaller fi the buffer/base level is higher. The current place of urea kinetic modeling with respect to different dialysis modalities. L-lactate high-effciency hemodialysis: Hemodynamics, blood gas changes, potassium/phosphorus, and symptoms. Cerebral dysfunction and respiratory alkalosis during peritoneal dialysis with D-lactate containing dialysis fuids. Lactateor bicarbonate buffered solutions in continuous extracorporeal renal replacement therapies. The effect of lactate buffered solutions on the acid-base status of patients with renal failure. Effect of frequent or extended hemodialysis on cardiovascular parameters: a meta-analysis. It calls attention to an operating No part of this manual may be reproduced in any form or by any procedure, practice, or the like that, if not correctly performed or means (including electronic storage and retrieval or translation into a adhered to , could result in damage to the product or loss of important foreign language) without prior agreement and written consent from data. It calls attention to an Edition operating procedure, practice, or the like that, if not correctly Fourteenth edition, May 2017 performed or adhered to , could result in personal injury or death. Do not use perchloric acid unless it is absolutely essential for sample preparation. If perchloric acid must be used, it may be possible to reduce the risk of an explosion by taking the following measures: fi Use an air-acetylene flame instead of a nitrous oxide-acetylene flame. The concentration of perchloric acid should be reduced in the digestion stage and further reduced by extending the fuming stage. In addition, if the organic solution is aspirated whilst floating on the surface of the acid, do not allow the capillary tube to drop below the organic solvent and suck up aqueous perchloric acid. Flame Atomic Absorption Spectrometry Analytical Methods 3 this page is intentionally left blank. Introduction 11 Interferences 18 References 18 General 11 As (Arsenic) 18 Safety Aspects 11 Recommended Instrument Reagents and Apparatus 12 Parameters 18 Sample Preparation 12 Interferences 19 References 19 Standard Preparation12 Au (Gold) 19 Automation 13 Recommended Instrument Matrix Effects 13 Parameters 19 Precipitation 13 Interferences 19 Physical Properties of B (Boron) 20 Standard and Sample 13 Recommended Instrument Parameters 20 Chemical Interferences 13 Interferences 20 Incomplete Dissociation of Ba (Barium) 20 Compounds 13 Ionization 14 Recommended Instrument Parameters 20 Nebulizers 15 Interferences 21 Organic Solvents15 Be (Beryllium) 21 Adjustable Recommended Instrument Nebulizer 15 Parameters 21 Spray Chamber 15 Interferences 21 Recommended Instrument References 21 Parameters 15 Bi (Bismuth) 21 Working Conditions Recommended Instrument (Fixed) 15 Parameters 21 Working Conditions Interferences 22 (Variable) 15 Vapor Generation General References 16 Method 22 References 22 2. Standard Conditions17 Ca (Calcium) 22 Ag (Silver) 17 Recommended Instrument Recommended Instrument Parameters 22 Parameters 17 Interferences 22 Interferences 17 References 23 Al (Aluminium) 17 Cd (Cadmium) 23 Flame Atomic Absorption Spectrometry Analytical Methods 5 Contents Recommended Instrument References 28 Parameters 23 Ga (Gallium) 29 Interferences 23 Recommended Instrument Co (Cobalt) 23 Parameters 29 Recommended Instrument Interferences 29 Parameters 23 Gd (Gadolinium) 29 Interferences 24 Recommended Instrument References 24 Parameters 29 Cr (Chromium) 24 Interferences 30 Recommended Instrument Ge (Germanium) 30 Parameters 24 Recommended Instrument Interferences 24 Parameters 30 References 25 Interferences 30 Cs (Cesium) 25 Hf (Hafnium) 30 Recommended Instrument Recommended Instrument Parameters 25 Parameters 30 Interferences 25 Interferences 31 Cu (Copper) 25 Hg (Mercury) 31 Recommended Instrument Recommended Instrument Parameters 25 Parameters 31 Interferences 26 Interferences 31 Dy (Dysprosium) 26 References 31 Recommended Instrument Ho (Holmium) 32 Parameters 26 Recommended Instrument Interferences 26 Parameters 32 References 26 Interferences 32 Er (Erbium) 27 In (Indium) 32 Recommended Instrument Recommended Instrument Parameters 27 Parameters 32 Interferences 27 Interferences 32 References 27 Ir (Iridium) 33 Eu (Europium) 27 Recommended Instrument Recommended Instrument Parameters 33 Parameters 27 Interferences 33 Interferences 28 References 33 References 28 K (Potassium) 34 Fe (Iron)28 Recommended Instrument Recommended Instrument Parameters 34 Parameters 28 Interferences 34 Interferences 28 6 Flame Atomic Absorption Spectrometry Analytical Methods Contents La (Lanthanum) 34 Recommended Instrument Recommended Instrument Parameters 40 Parameters 34 Interferences 40 Interferences 35 Os (Osmium) 40 Li (Lithium) 35 Recommended Instrument Recommended Instrument Parameters 40 Parameters 35 P (Phosphorus) 41 Interferences 35 Recommended Instrument Lu (Lutetium) 35 Parameters 41 Recommended Instrument Interferences 41 Parameters 35 References 41 Interferences 36 Pb (Lead) 41 References 36 Recommended Instrument Mg (Magnesium) 36 Parameters 41 Recommended Instrument Interferences 42 Parameters 36 Pd (Palladium) 42 Interferences 36 Recommended Instrument References 37 Parameters 42 Mn (Manganese) 37 Interferences 42 Interferences 37 References 42 Mo (Molybdenum) 37 Pr (Praseodymium) 42 Recommended Instrument Recommended Instrument Parameters 37 Parameters 42 Interferences 38 Interferences 43 References 38 Pt (Platinum) 43 Na (Sodium) 38 Recommended Instrument Parameters 43 Recommended Instrument Parameters 38 Interferences 43 Interferences 38 References 44 Nb (Niobium) 38 Rb (Rubidium) 44 Recommended Instrument Recommended Instrument Parameters 38 Parameters 44 Interferences 39 Interferences 44 References 39 Re (Rhenium) 44 Nd (Neodymium) 39 Recommended Instrument Parameters 44 Recommended Instrument Parameters 39 Interferences 45 Interferences 39 Rh (Rhodium) 45 Ni (Nickel) 40 Flame Atomic Absorption Spectrometry Analytical Methods 7 Contents Recommended Instrument Recommended Instrument Parameters 45 Parameters 50 Interferences 45 Interferences 50 References 45 References 50 Ru (Ruthenium) 46 Ta (Tantalum) 51 Recommended Instrument Recommended Instrument Parameters 46 Parameters 51 Interferences 46 Interferences 51 References 46 References 51 Sb (Antimony) 46 Tb (Terbium) 51 Recommended Instrument Recommended Instrument Parameters 46 Parameters 51 Interferences 47 Interferences 52 Vapor Generation The (Tellurium) 52 Method 47 Recommended Instrument References 47 Parameters 52 Sc (Scandium) 47 Interferences 52 Recommended Instrument Vapor Generation Parameters 47 Method 52 Interferences 47 References 52 References 48 Ti (Titanium) 53 Se (Selenium) 48 Recommended Instrument Recommended Instrument Parameters 53 Parameters 48 Interferences 53 Interferences 48 References 53 References 48 Tl (Thallium) 53 Si (Silicon) 48 Recommended Instrument Recommended Instrument Parameters 53 Parameters 48 Interferences 53 Interferences 49 Tm (Thulium) 54 Sm (Samarium) 49 Recommended Instrument Recommended Instrument Parameters 54 Parameters 49 Interferences 54 Interferences 49 V (Vanadium) 54 Sn (Tin) 49 Recommended Instrument Recommended Instrument Parameters 54 Parameters 49 Interferences 55 Interferences 50 References 55 References 50 W (Tungsten) 55 Sr (Strontium) 50 8 Flame Atomic Absorption Spectrometry Analytical Methods Contents Recommended Instrument References 64 Parameters 55 Barium Standard Interferences 55 Conditions 64 References 55 Method 1 64 Method 2 65 Y (Yttrium) 56 Recommended Instrument 4. Introduction General 11 Safety Aspects 11 Reagents and Apparatus 12 Sample Preparation 12 Standard Preparation 12 Automation 13 Matrix Effects 13 Chemical Interferences 13 Nebulizers 15 Organic Solvents 15 Recommended Instrument Parameters 15 General References 16 General Safety Aspects this book is intended as a guide to analysts in Some warning messages will appear in the the selection of techniques and instrument text. Consequently, where analytical in any doubt over the correct handling circumstances differ appreciably from those procedures for any material, you should indicated in the book, appropriate changes in consult an appropriate reference on the operating conditions may be required. Throughout the book, emphasis had been You should also observe the warning on placed on practical applications and no Page 3 of this book, and refer to Reference 8 attempt has been made to provide a complete (at the end of this section). Also, while every effort has been made to fi Buildup of salt or carbon deposits on a ensure the validity of the published material burner should never be allowed to in this book, analysts should satisfy continue unchecked. Flame Atomic Absorption Spectrometry Analytical Methods 11 Introduction Solvent extraction can also be used to remove Reagents and Apparatus a major element and reduce the overall the purity of reagents may determine the solution concentration. In iron and steel accuracy of the analysis and all reagents analysis, ketone or ester extraction from should therefore be of the highest purity strong hydrochloric acid solution removes available. This Prior to any analysis all reagents and eases the requirements for matrix matching equipment should first be checked for the of standards. When choosing a solvent for organic extraction, avoid using aromatics such as All apparatus for trace analysis should be benzene, or highly volatile halogen solvents thoroughly soaked in dilute nitric acid and such as carbon tetrachloride and chloroform. It is recommended that a full set of types of solvent will create severe flame new apparatus be put aside expressly for use disturbance. Methyl available and should be used in preference to isobutyl ketone, diisobutyl ketone and ethyl glass whenever hydrofluoric acid or strong acetate are the solvents most commonly used caustic solutions are to be handled. The sample to be analyzed can be brought Detailed methods for solvent extraction of into solution by a number of means: metals can be found in the literature. This automatically fi dissolution in solvent compensates for the slight solubility of Whichever procedure is used, it is essential to solvents in water, the extraction efficiency ensure that no analyte element is lost and involved (which is rarely 100%), and any that a clear, stable solution is obtained. When carrying out dissolution it is advisable to avoid adding components likely to cause Standard Preparation severe interference. For example, in the alkali fusion of tantalum ores, potassium should not Agilent offers a comprehensive range of single be used since it will form highly refractory and multi-element standards, tuning potassium fluorotantalate. In atomic absorption analysis solution is manufactured using high purity this is generally achieved by solvent starting materials, which are regularly tested extraction. Note that solutions at low concentrations the formation of ground state atoms can be (less than 10 fig/mL) have been found to inhibited by two general forms of chemical deteriorate quite quickly because of interferences. Such interferents both of which can automate many tedious and form compounds which are not completely error prone sample preparation tasks. It is also use the following method to check for small, quiet, easy-to-use and affordable. Matrix Effects Precipitation Inaccurate results are commonly caused by precipitation of the element of interest. Examples of this are: the hydrolysis of silicon and tin compounds, and the formation of insoluble chlorides and sulfates. To avoid differences changes in the absorbance of the analyte in the amount of sample and standard which element. Because this is analytically reach the flame, it is necessary that the undesirable, the analyst should use a sample physical properties of sample and standard treatment procedure which will avoid be matched as closely as possible. Flame Atomic Absorption Spectrometry Analytical Methods 13 Introduction Where interference is encountered, the Extract the Interferent following procedure for optimization of the It is often possible to remove the interferent flame stoichiometry is recommended: by organically extracting if from solution. A 1 Prepare two calibration standards having highly specific and quantitative extraction is the same analyte element concentration not always necessary. This allows 2 Light the flame and measure the trace analysis to be carried out on the absorbance of both solutions. For example, in stoichiometry and minimize the effects of calcium determinations, lanthanum or interference to yield improved accuracy and strontium nitrate can be added to solutions precision. This will allow If interference is still present and cannot be calcium to be determined in an air-acetylene compensated for, then 4 means of overcoming flame without interference due to the it are possible: formation of calcium phosphate. Use a Higher Temperature Flame Ionization Where compounds are insufficiently High temperature flames such as nitrous dissociated in the cooler flames, a high oxide/acetylene may cause appreciable temperature flame such as nitrous oxideionization of the analyte element. The alkali acetylene can frequently supply sufficient and alkaline-earth metals are more thermal energy to cause complete susceptible to ionization than the transition dissociation. The addition of readily ionized Extract the Analyte Element elements such as sodium, potassium and Where the interference assumes serious cesium at concentrations between 2000 and proportions, it is sometimes possible to 5000 fig/mL creates an excess of electrons in extract the analyte element into an organic the flame and effectively suppresses medium. For example, suppressant concentration against analyte potassium interference on tantalum can be absorbance as shown. Adjustable Nebulizer Some typical ionization potentials are: When an organic solvent is analyzed by flame atomic absorption spectrometry, it effectively contributes extra fuel to the flame. It is Metal Ionization Potential (eV) recommended that an adjustable nebulizer is Al 6. It is ionization will vary with the concentration of therefore desirable to examine the effect of the analyte element. When using more flame conditions (or stoichiometry) on the concentrated solutions (as for example when signal. An oxidizing flame is one with low operating on alternative wavelengths), acetylene content, while a reducing flame has ionization may not present a serious problem. The nebulizer and glass bead can be set to Working Conditions (Variable) achieve the desired analytical performance dictated by your sample type. For example, the upper limit of the working range they may be set to achieve a high absorbance concentration will give about 0. Refer to the range is about 10 times the defined detection appropriate Agilent documentation for limit. Flame Atomic Absorption Spectrometry Analytical Methods 15 Introduction the alternative wavelengths shown have been selected to give a variety of working ranges. However, the sensitivities are no better than the listed lines and the latter have been preferred because of the relatively better signal strength and spectral purity. Flame Atomic Absorption Spectrometry Analytical Methods 17 Standard Conditions Aluminium emission appears in the center of 3. Major factors in the determination at low levels of detection are the adjustment of fuelsupport ratio and burner height. The use of flame emission is only recommended for very low concentrations of aluminium in solutions of simple aqueous matrix. Interferences Aluminium is partially ionized in the nitrous oxide-acetylene flame. To suppress ionization, add potassium nitrate or chloride to give final concentration of 2000 fig/mL potassium. The addition of a readily ionizable element such as potassium overcomes enhancement As (Arsenic) interference from other alkali metals. Support nitrous oxide this non-atomic absorption can be corrected by means of a continuum light source such as Interferences a deuterium lamp. The nitrous oxide-acetylene flame will remove any interference but provides a lower sensitivity. The effect is usually minimized by adjusting the flame to neutral stoichiometry (red cone 0. To suppress ionization, 1000 fig/mL have been found to severely add potassium nitrate or chloride solution to depress beryllium absorbance. This was the strong emission from barium falling on overcome by the presence of 1. Details of the appropriate procedures are given in the operation manual Wavelength 422. Interferences Chemical interferences in the air-acetylene flame are pronounced and have been fairly well documented(1,2,3,4). These interferences, which depress the calcium absorbance, can be eliminated by the introduction of a releasing agent such as strontium (5000 fig/mL) or lanthanum (10000 fig/mL). Normally the addition of a releasing agent is used in conjunction with the practice of matching sample and standard solutions to obviate combined interference effects. Interferences No major chemical interference has been reported in the air-acetylene flame. Support air Note 2: Absorbance strongly dependent on Flame stoichiometry oxidizing flame stoichiometry. Flame Atomic Absorption Spectrometry Analytical Methods 23 Standard Conditions Working Conditions (Variable) Cr (Chromium) Wavelength Slit Width Optimum Working A. Support nitrous oxide Interferences Cobalt, iron and nickel (particularly in the presence of perchloric acid) have been found to cause depression of chromium absorbance. This can be overcome using an oxidizing airacetylene flame or preferably a nitrous oxideacetylene flame. Several authors(1, 2, 3) have found interference in air-acetylene flame from copper, barium, aluminium, magnesium and calcium. Optimization of the stoichiometry or the use of the nitrous oxide-acetylene flame can eliminate the interference. This can be minimized by the use of a concentrations, atomic absorption is normally lean air-acetylene flame or a nitrous oxideused. Interferences Hydrofluoric acid, aluminium and silicon have been found to depress the absorbance by 90%. Interferences of this type can usually be overcome by the precipitation of the rare earth oxide and subsequent dissolution in dilute hydrochloric acid. To suppress ionization, Dy (Dysprosium) add potassium nitrate or chloride solution to give a final concentration of 4000 fig/mL A. To suppress ionization, add potassium nitrate or chloride solution to give a final concentration of 4000 fig/mL potassium in all solutions including the blank. Fuel acetylene Interference may be minimized by the Support air precipitation of the rare earth oxide and subsequent dissolution in hydrochloric acid.
Triangular gap near the posterior commissure (interaryfi Functional Type: Voice therapy and psychological counseling medicine 8 capital rocka discount norpace 100mg with mastercard. Keyhole appearance of glottis due to combination of functional aphonia (hySterical both elliptical space between the cords and triangular aphonia) gap near the posterior commissure (weakness of both fi this functional disorder is usually seen in emotionally labile thyroarytenoid and interarytenoid) medicine 93 3109 buy 100mg norpace. The adduction of vocal cords occurs on coughing resonance for words and is called hyponasality medicine go down buy norpace 150 mg lowest price. After puberty medications in mothers milk purchase norpace on line, nasal resonance of all the words (even those words medicine examples purchase norpace australia, which have male larynx grows rapidly treatment receding gums order 100 mg norpace with mastercard. Short soft palate: Congenital or acquired (submucous fi Occasionally, compensatory pseudoabductor spasmodic fbrosis) dysphonia compensates for severe adductor laryngeal Cleft palate or submucous cleft palate spasms by whispering. Paralysis of soft palate Palatal perforation abductor Spasmodic dysphonia Large nasopharynx Abnormal co-contraction of the posterior cricoarytenoid After adenoidectomy muscles results in inappropriate abduction of the vocal cords. SpaSmodic dySphonia Dystonia is characterized by abnormal involuntary movements, treatment which are typically action induced. Spasmodic dysphonia, fi Voice therapy focal dystonia of larynx is an action induced laryngeal motion fi Alcohol, sedatives and tranquilizers provide transient disorder. Vocal tremor types the involuntary, rhythmic and oscillatory movements can afect There are three types of spasmodic dysphonia: adductor, the muscles of speech production and generate rhythmic alterabductor and mixed. Adductor is caused by irregular hyperadduction of the vocal or wavy voice or tremulous quavering speech. Abductor is caused by intermittent abduction of the vocal clinical features folds. Mixed type displays a combination of adductor and fi Vocal tremor can result in rapid decreases and increases in abductor signs. Stuttering Stuttering is a neurologic, movement disorder in which abnormal, adductor Spasmodic dysphonia involuntary, and inappropriate use of the speech muscles results Abnormal involuntary co-contraction of the vocalis muscle in dysfuency. Stuttering is a result of increased muscle tension complex results in inappropriate adduction of the vocal folds. Other cranial musculature (such as eyelids and muscles of facial expression) may fi Vocal cords often show slow rhythmic adduction and 499 also inappropriately contract. Lingual tics present as fi Singing or speaking in a sing-song voice hisses and nasal tics as snifs and snorts. The factors, which may increase stuttering, include communifi Laryngeal tics: Inappropriate coughing, barking, throat cative pressures such as public speeches, personal interviews, clearing, hooting and grunting. Injection botulinum toxin is said to be a safe and efective therapy for laryngeal dystonia. It consists inhibiting the release of acetylcholine and causes a faccid of sudden, brief, shock like involuntary movements, which are paralysis. The steps involved in toxin-mediated paralysis are caused by either muscular contractions (positive myoclonus) binding, internalization and inhibition of neurotransmitter or inhibitions (negative myoclonus, asterixis). The clinical efect of toxin is caused mainly by the peripheral laryngeal features efect. The degree of improvement correlates with weakness fi Broken speech pattern and respiratory dysrhythmia (ventiladue to blockade of neuromuscular transmission. The needle is advanced to the cricoid cartivarious concentrations, as per the need and the indication. The needle is placed adductor laryngeal injections through the cricothyroid membrane, traversing the airway until it engages the posterior lamina of the cricoid cartilage. The posterior cricoarytenoid fi Percutaneous: They are performed percutaneously through muscle is encountered and snifng shows a burst of electric the cricothyroid membrane and into the thyroarytenoidpotentials. If there is no fi Side Efects: Patients report improvement in voice within 24 impairment in motion, repeat the injection. The contralateral injection is Occasionally causing hyperventilation and dizziness given only after the return of function on the injected when trying to speak. Wernicke aphasia (sensory or fuent aphasia): Patient cannot comprehend the spoken word. Patient looks at the doctor as if s/he does not understand what the doctor is saying. The lesion of this limited language defcit is in the arcuate fasciculus, which connects the Wernicke and Broca areas. The pressure relaxes the over-stretched vocal cords and low-pitched voice can be produced. Take the whole responsibility on your own shoulders, and know that you are the creator of your own destiny. Indians are Alcohol and smoking together increase the risk many-fold, afected more than the people in Western countries. Patients are mostly in the age group of lower risk than fue-cured or black tobacco. Impairment or fxation occurs 502 fi Radiation: Previous radiation to neck such as radiation for due to infltration of thyroarytenoid muscle, cricoarytenoid laryngeal papilloma may induce laryngeal carcinoma. It is an important fnding fi Familial: Japanese and Russian workers have familial larynfor staging, management and prognosis of laryngeal cancer. Lymph node metastasis: Note the size and number; fi Genetic: Either inactivation of tumor suppressive genes whether mobile or fixed and unilateral, bilateral or or activation of proto-oncogenes occurs. Note the widening of thyroid cartilage and healed with airway obstruction without any history of hoarseness tracheostomy opening of voice. Thyroid or cricoid cartilage destruction tions for emergency tracheostomy should be kept ready. Imaging of the neck and airway before biopsy and operative endoscopy recognizes the need for emergent tracheostomy. It provides better view of the extent of disease and certain hidden areas, which are not seen during mirror examination detection of recurrent/residual disease such as infrahyoid epiglottis, anterior commissure, subglottis Early recognition becomes difficult due to mucositis and and ventricle. Telescopes may be passed through the scope for edema of supraglottic laryngeal structures. The following imaging methods help: fi Microlaryngoscopy: Small lesions of vocal cords are better 1. Cord fxation is diferentiated from arytenoid fxation by palpating the vocal process. The ventricular extension of differential diagnoses growth is assessed with a laryngeal probe. The complete excisional biopsy of small suspected lesion the gross appearance of following conditions may be mistaken with border of healthy tissue helps in determining the depth for malignancy. So, it helps in selecting Indirect laryngoscopy the area for biopsy in cases of leukoplakia. Other variants of squamous cell carcinoma include the following: fi Verrucous carcinoma fi Pseudosarcoma fi Basaloid squamous cell carcinoma. Rare laryngeal malignancies are the following: fi Sarcomas fi Lymphoma fi Adenocarcinoma fi Neuroendocrine carcinoma fi Extramedullary plasmacytoma. Laryngeal cancer: the most common malignancy of the larynx is squamous cell carcinoma. Squamous cell carcinoma with various grades of differentiation accounts for 95% of all laryngeal malignancies. T4a Tumor invades thyroid cartilage and any of the (A) Supraglottic; and (B) Glottic following extralaryngeal structures: esophagus, trachea, thyroid, infrahyoid strap muscles, or fi Supraglottis: Suprahyoid epiglottis (both lingual and laryngeal tongue muscles surfaces), infrahyoid epiglottis, aryepiglottic folds (laryngeal T4b Tumor involves prevertebral space, mediastinum aspect only), arytenoids, ventricular bands (or false cords). The staging and T1b Tumor involves both vocal cords with normal vocal cord mobility classifcation help to analyze outcomes of diferent modalities of treatment, and assists in predicting prognosis of disease. The modalities of treatment include radiotherapy, T4a Tumor invades thyroid cartilage and any of the surgery (conservation and total laryngectomy), chemotherapy following extralaryngeal structures: esophagus, and combined therapy. The cords or encasing of carotid artery are mobile, and there is no involvement of cartilage and cervical Subglottis nodes. T1 Tumor limited to subglottis with normal vocal In cases of vocal cord cancer, radiotherapy gives 90% cure rate. T2 Tumor spreads to glottis with or without impaired vocal cord mobility the results are not good in cases of fxed cords, subglottic extension, cartilage invasion, and nodal metastases. These cases T3 Tumor limited to larynx with vocal cord fxation are candidates for surgery. T4a Tumor invades cricoid or thyroid cartilage and any of the following extralaryngeal structures: Surgery esophagus, trachea, thyroid, infrahyoid strap muscles, or tongue muscles To prove negative surgical margins, the specimen should be T Tumor involves prevertebral space, mediastinum 4b submitted for histopathological examination. T4a Tumor invades any of the following: thyroidcricoid cartilage, hyoid bone, thyroid gland, esophagus, central compartment of soft tissue such as infrahyoid strap muscles and subcutaneous tissue. T4b Tumor involves prevertebral fascia, mediastinum or encasing of carotid artery Regional lymph nodes (N) size in greatest dimension Nx Cannot be assessed Fig. Note the incision and skin changes after N Single ipsilateral node > 3 cm but fi 6 cm postoperative radiotherapy 2a N2b Multiple ipsilateral nodes but none > 6 cm associated hemithyroidectomy or subtotal thyroidectomy N2c Bilateral or contralateral nodes but none > 6 cm is indicated in following conditions: N3 Any node > 6 cm Palpable thyroid abnormality Subglottic extension or tumors Distant metastasis (M) T glottic tumors M Cannot be assessed 4 x T pyriform sinus tumors 4 M0 No distant metastasis Positive Delphian nodes M1 Distant metastasis Cartilage destruction Stage grouping combined therapy Stage 0 this N0 M0 Surgery may be combined with pre or postoperative radiaSatge I T1 N0 M0 tion in a planned way to decrease the incidence of recurrence. Partial frontolateral laryngectomy: Excision of vocal cord this is the most common laryngeal cancer with good prognosis and anterior commissure. Partial horizontal laryngectomy: Excision of supraglottis, most common sites are free edge and upper surface of vocal which include epiglottis, aryepiglottic folds, false cords cord in its anterior and middle third. It is combined with Posterior: Vocal process and arytenoid region block dissection when nodal metastasis is present. It is not Upward: Ventricle and false cord done in patients with distant metastasis. Downward: Subglottic region fi Hemithyroidectomy or Subtotal Thyroidectomy: the fi Lymphatic: There are not much lymphatic in vocal cords. Cord ventricular band extend into preepiglottic space, and cancer afects vibratory capacity. If biopsy B) remain silent for long time till they achieve enormous size reveals invasive carcinoma, radiotherapy is given. But, fi Late symptoms: radiotherapy failures may not be amenable to conserHoarseness of voice vation surgery. Infrahyoid epiglottic tumors: Endoscopic laser partial In a case of postradiation edema, which persists for longer laryngectomy. In cases Vallecula and base of tongue up to the circumvallate of radiation failure, laryngectomy or partial vertical papilla can be removed. Anterior commissure and/or arytenoids involved or cord mobility impaired: Vertical hemi-laryngectomy or frontolateral laryngectomy. Apollo Hospital, Ahmedabad mild-to-moderate aspiration that may last for the rest radiotherapy, they may undergo transformation to undifer507 of life. The current trend in the management of cancer of larynx fi T3 and T4: Total laryngectomy with neck dissection and is developing towards chemotherapy+radiotherapy for postoperative radiotherapy. Studies have shown that there is no diference in survival rate between the cases of total laryngecSubglottIc cancEr tomy and combined chemotherapy+radiotherapy. Subglottic region lies below the glottic area, and extends up to the patients who are candidates for total laryngectomy are the lower border of cricoid cartilage. Those who have no response (some Spread include even partial response) are treated with surgery, usually followed by radiotherapy. No diference in survival was found fi Local: One side growth of subglottis spreads around the in these two groups; those who went for radiotherapy or anterior wall, and to the opposite side. Superfcial cancers of larynx have been fi Stridor: the most common symptom is airway obstruction. Erythrocyte treatment leakage and endothelial damage of vessels cause ischemic necrosis of tumor tissue. Failure Artifcial larynx is useful when patients fail to learn esophageal to complete excision, results in local recurrence. They are least socially acceptable because they draw 508 unwanted attention to the speaker. Monotone sound producshunts the air from trachea to esophagus, and their inbuilt tion is another limitation of artifcial larynx. The vibrating disc of artifcial larynx is held fi Prosthesis: There are two types of prostheses non-indwelling against the soft tissues of the neck or oral cavity. These rubber diaphragm vibrations are carried remove them daily for cleaning and maintenance. They by a plastic tube into the back of the oral cavity where include: modulators convert the sound into speech. In case of problems they the air is carried from trachea to esophagus/hypopharynx are replaced by the therapist or surgeon. Blom-Singer Indwelling Voice Prosthesis (InHealth patients who use esophageal speech. In comparison to supraglottis, nasopharynx and subglottic cancers, carcinoma glottis is the most radiosensitive tumor.
The difference medicine 54 357 purchase norpace 100 mg overnight delivery, p1 A p0 medications given during dialysis buy norpace 150 mg with visa, between the proportions in the exposed and unexposed groups in our sample provides an estimate of the underlying difference medicine app purchase 150 mg norpace otc, 1 A 0 medicine 2000 buy norpace online, between the exposed and unexposed groups in the population medicine lodge ks generic 100mg norpace otc. It is of course subject to sampling variation symptoms thyroid cheap 150mg norpace otc, so that a different sample from the same population would give a different value of p1 A p0. Note that: 1 the normal distribution is a reasonable approximation to the sampling distribution of the difference p1 A p0, provided n1p1, n1 A n1p1, n0p0 and n0 A n0p0 are each greater than 10, and will improve as these numbers get larger. Test that the difference between two proportions is zero the normal test to compare two sample proportions is based on: p1 A p0 z fi s:e:(p1 A p0) the standard error used in the test is different to that used in the confidence interval because it is calculated assuming that the null hypothesis is true. Under the null hypothesis that the population proportions are equal: p s:e:(p1 A p0) fi [ (1 A)(1=n1 fi 1=n0)] is estimated by the overall proportion in both samples, that is by: d0 fi d1 d p fi fi n0 fi n1 n 16. If this condition is not satisfied, but n1p, n1 A n1p, n2p and n2 A n2p are all 5 or more, then a modified version of the z-test incorporating a continuity correction, or the equivalent chi-squared test with a continuity correction, can be used (see Section 17. If none of these conditions are satisfied, the exact test described in Section 17. Therefore: (0:083 A 0:364) A0:281 z fi p fi fiA7:299 fi 0:217(1 A 0:217)(1=240 fi 1=220) 0:0385 the corresponding P-value is < 0:0001. Thus there is strong evidence that there was a reduction in the risk of contracting influenza following vaccination with the influenza vaccine. We will refer to this as the risk ratio, although the methods apply to ratios of any proportions, and not just those that estimate risks. Thus the risk of lung cancer was considerably higher among smokers than nonsmokers. Lung cancer No lung cancer Total Risk Smokers 39 29961 30000 p1 A 39=30000 fi 0:0013 (0:13%) (exposed) Non-smokers 6 59994 60000 p0 A 6=60000 fi 0:0001 (0. A risk ratio greater than 1 occurs when the risk of the outcome is higher among those exposed to the factor (or treatment) than among the non-exposed, as in Example 16. A risk ratio less than 1 occurs when the risk is lower among those exposed, suggesting that the factor (or treatment) may be protective. An example is the reduced risk of infant death observed among infants that are breast-fed compared to those that are not. The further the risk ratio is from 1, the stronger the association between exposure (or treatment) and outcome. Relationship between risk ratios and risk differences the risk ratio is more commonly used to measure of the strength of an association than is the difference in risks. The use and interpretation of ratio and difference measures of the size of exposure effects is discussed in Chapter 37. To overcome this problem, we adopt the following procedure: 1 Calculate the logarithm of the risk ratio, and its standard error. The formula for this standard error is derived using the delta method (see Box 16. This is a technique for calculating the standard error of a transformed variable from the mean and standard error of the original untransformed variable. In this Box, we briefly outline how this method is used to give (a) an approximate formula for the standard error of a log transformed variable, and in particular (b) the formula for the standard error of a log transformed proportion. We then show how this result can be used to derive (c) an approximate formula for the standard error of the log(risk ratio). This approximation works provided that the variance of variable X is small compared to its mean. Further analyses of risk ratios the risk ratio is a measure that is easy to interpret, and the analyses based on risk ratios described in this chapter are straightforward. Perhaps surprisingly, however, more complicated analyses of associations between exposures and binary outcomes are rarely based on risk ratios. It is much more common for these to be based on odds ratios, as discussed in the next section, and used throughout 16. Both the prevalence (proportion with asthma) and odds of asthma in women and men are shown, as are their ratios. In this example the odds ratio is close to the ratio of the prevalences; this is because the prevalence of asthma is low (6% to 8%). An odds ratio of 1 occurs when the odds, and hence the proportions, are the same in the two groups and is equivalent to no association between the exposure and the disease. The odds ratio is always further away from 1 than the corresponding risk (or prevalence) ratio. The odds ratio for the occurrence of disease is the reciprocal of the odds ratio for non-occurrence. The odds ratio for exposure, that is the odds of disease in the exposed compared to the odds in the unexposed group, equals the odds ratio for disease, that is the odds of exposure in the disease compared to the odds in the healthy group. In contrast, interpretation of odds ratios often causes problems; except for gamblers, who tend to be extremely familiar with the meaning of odds (see Chapter 14). Odds ratio fi 2 Risk ratio fi 2 Risk in the Corresponding Risk in the Corresponding unexposed group risk ratio unexposed group odds ratio 0. A common mistake in the literature is to interpret an odds ratio as if it were a risk ratio. For rare outcomes, this is not a problem since the two are numerically equal (see Box 16. However, for common outcomes, this is not the case; the interpretation of odds ratios diverges from that for risk ratios. When the outcome is common, therefore, an odds ratio of (for example) 2 or 5 must not be interpreted as meaning that the risk is multiplied by 2 or 5. As the risk in the unexposed group becomes larger, the maximum possible value of the risk ratio becomes constrained, because the maximum possible value for a risk is 1. Note that as the risk in the unexposed group increases the odds ratio becomes much larger than the risk ratio and, as explained above, should no longer be interpreted as the amount by which the risk factor multiplies the risk of the disease outcome. The constraint on the value of the risk ratio can cause problems for statistical analyses using risk ratios when the outcome is not rare, because it can mean that the risk ratio differs between population strata. A further difficulty with risk ratios is that the interpretation of results may depend on whether the occurrence of an event, or its non-occurrence, is considered as the outcome. For instance, consider the low-risk stratum in which the risk ratio is 0:5=0:2 fi 2:5. If the nonoccurrence of disease (healthy) is considered as the outcome, then the risk ratio is (1 A 0:5)=(1 A 0:2) fi 0:5=0:8 fi 0:625. The risk of severe nausea is 88% in the group treated with the new drug and 71% in the group given standard treatment, so the risk ratio is 0:88=0:71 fi 1:239, an apparently moderate increase in the prevalence of nausea. Note, however, that the risk ratio is constrained: it cannot be greater than 1=0:71 fi 1:408. The risk ratio is 0:12=0:29 fi 0:414: the proportion of patients without severe nausea has more than halved. Number with Number without severe nausea severe nausea Total New drug 88 (88%) 12 100 Standard treatment 71 (71%) 29 100 Rationale for the use of odds ratios In the recent medical literature, the statistical analysis of binary outcomes is almost always based on odds ratios, even though they are less easy to interpret than risk ratios (or risk differences). This is because the odds of occurrence of a rare outcome are numerically equivalent to its risk. Analyses based on odds ratios therefore give the same results as analyses based on risk ratios. Analyses based on risk ratios, particularly those examining the effects of more than one exposure variable, can cause computational problems and are difficult to interpret. Taken together, these mean that analyses of binary outcomes controlling for possible confounding (see Chapter 18), or which use regression modelling (see Chapters 19 to 21), usually report exposure effects as odds ratios, regardless of whether the outcome is rare or common. The distribution of one or more exposures in the cases is then compared with the distribution in the controls. Confidence intervals for the odds, and the odds ratio, are calculated in exactly the same way. The categories for one variable define the rows, and the categories for the other variable define the columns. Individuals are assigned to the appropriate cell of the contingency table according to their values for the two variables. A contingency table is also used for discrete numerical variables, or for continuous numerical variables whose values have been grouped. These larger tables are generally called r A c tables, where r denotes the number of rows in the table and c the number of columns. If the variables displayed are an exposure and an outcome, then it is usual to arrange the table with exposure as the row variable and outcome as the column variable, and to display percentages corresponding to the exposure variable. In this chapter, we describe how to use a chi-squared (x2) test to examine whether there is an association between the row variable and the column variable or, in other words, whether the distribution of individuals among the categories of one variable is independent of their distribution among the categories of the other. When the table has only two rows and two columns the x2 test is equivalent to the z-test for the difference between two proportions. We also describe the exact test for a 2 A 2 table when the sample size is too small for the z-test or the x2 test to be valid. Since the exposure is vaccination (the row variable), the table includes row percentages. We now wish to assess the strength of the evidence that vaccination affected the probability of contracting influenza. Overall 100/460 people contracted influenza and, if the vaccine and the placebo were equally effective, one would expect this same proportion in each of the two groups; that is 100=460 A 240 fi 52:2 in the vaccine group and 100=460 A 220 fi 47:8 in the placebo group would have contracted influenza. Similarly 360=460 A 240 fi 187:8 and 360=460 A 220 fi 172:2 would have escaped influenza. The chi-squared value is obtained by calculating 2 (observed A expected) =expected for each of the four cells in the contingency table and then summing them. The greater the differences between the observed and expected numbers, the larger the value of x2. The percentage points of the chi-squared distribution are given in Table A5 in the Appendix. The values depend on the degrees of freedom, which equal 1 for a 2 A 2 table (the number of rows minus 1 multiplied by the number of columns minus 1). In this example: 2 2 2 2 2 (20 A 52:2) (80 A 47:8) (220 A 187:8) (140 A 172:2) fi fi fi fi 52:2 47:8 187:8 172:2 fi 19:86 fi 21:69 fi 5:52 fi 6:02 fi 53:09 53. Thus there is strong evidence against the null hypothesis of no effect of the vaccine on the probability of contracting influenza. Relation with normal test for the difference between two proportions the square of the z statistic (normal test) for the difference between two proportions and the chi-squared statistic for a 2 A 2 contingency table are in fact mathematically equivalent (x2 fi z2), and the P-values from the two tests are identical. Note that the percentage points given in Table A5 for a chi-squared distribution with 1 degree of freedom correspond to the two-sided percentage points presented in Table A2 for the standard normal distribution (see Appendix). The formula becomes: 2 2 (jO A EjA0:5) fi fi,d:f: fi 1 E resulting in a smaller value for x2. In the example the value for x2 becomes: 2 2 2 2 2 (32:2 A 0:5) (32:2 A 0:5) (32:2 A 0:5) (32:2 A 0:5) fi fi fi fi 52:2 47:8 187:8 172:2 fi 19:25 fi 21:02 fi 5:35 fi 5:84 fi 51:46, P < 0:001 compared to the uncorrected value of 53. It makes little difference unless the total sample size is less than 40, or the expected numbers are small. When the expected numbers are very small, then the exact test described in Section 17. Validity When the expected numbers are very small the chi-squared test (and the equivalent z-test) is not a good enough approximation and the alternative exact test for a 2 A 2 table should be used (see Section 17. Cochran (1954) recommended the use of the exact test when: 1 the overall total of the table is less than 20, or 2 the overall total is between 20 and 40 and the smallest of the four expected numbers is less than 5. Only one (8%) of the 13 haemophiliacs given treatment regime A suffered bleeding complications, compared to three (25%) of the 12 given regime B. These numbers are too small for the chi-squared test to be valid; the overall total, 25, is less than 40, and the smallest expected value, 1. In order to test the null hypothesis that there is no difference between the treatment regimes, we need to calculate not only the probability of the observed table but also the probability that a more extreme table could occur by chance. Altogether there are five possible tables that have the same row and column totals as the data. In the first approach, more extreme is defined as less probable; more extreme tables are therefore 17. The total probability needed for the P-value is therefore 0:2261 fi 0:0391 fi 0:0565 fi 0:3217, and so there is clearly no evidence against the null hypothesis of no difference between the regimes. In this example, the P-value thus obtained would be twice the sum of the probabilities of Tables 17. Neither method is clearly superior to the other, but the second method is simpler to carry out. Although the two approaches give different results, the choice is unlikely, in practice, to affect the assessment of whether the observed difference is due to chance or to a real effect. The chi-squared test can also be applied to larger tables, generally called r AAc tables, where r denotes the number of rows in the table and c the number of columns. Cochran (1954) recommends that the approximation of the chi-squared test is valid provided that less than 20% of the expected numbers are under 5 and none is less than 1. This restriction can sometimes be overcome by combining rows (or columns) with low expected numbers, providing that these combinations make biological sense. The general rule for calculating an expected number is: column total A row total E fi overall total It is worth pointing out that the chi-squared test is only valid if applied to the actual numbers in the various categories. We will treat the water source as outcome and village as exposure, so column percentages are displayed. If there were no difference between villages one would expect this same proportion of river usage in each village.
If one fraction (in this case symptoms 5 days post embryo transfer discount norpace 100mg fast delivery, the fat) is lowered medications drugs prescription drugs buy norpace 150mg lowest price, either one or both of the other two fractions must be increased treatment questionnaire cheap norpace online. In this case medicine 44334 buy generic norpace line, the pet food companies *should* raise the protein when the fat is lowered but that would cut into their profit margin so treatment neuropathy order norpace 100mg on line, instead symptoms dengue fever effective 100mg norpace, they increase the carbs which is a cheaper source of calories. Biological value of protein: Animal-based protein has a much higher biological value when compared to plant-based protein. Consider not only the amount of protein in a diet but also the source of the protein. Diets using whole grains or glutens (gluten = plant-based protein) have a portion of their protein coming from low biological value sources. Protein source: How do we know how much of the protein is coming from animals versus plants when an ingredient list includes both animal and plant (grains/potatoes/vegetables) protein sourcesfi This compounds the problem of grains contributing more to the protein level than the animal sources. Liver: I definitely want to see liver in the product since it is a wonderful source of nutrients (vitamin A and D, copper, zinc, etc. That said, not every meal has to contain liver but I like to see some liver fed several times/week. Cats have a hard enough time maintaining thyroid health (hyperthyroidism is extremely common in older cats) and soy is a known thyroid disruptor. Pouches are typically high in water making them more expensive on a $$/calorie basis. I suggest looking for products with a maximum water content of 78%, versus 82% or 85%. If you are interested in making your own cat food, see Making Cat Food for a detailed discussion regarding safe preparation and sourcing, along with a recipe that I have been feeding to my own cats since 2003. The peace of mind that comes with my control over ingredients, composition, and safety issues is priceless. This chart required hundreds of hours of phone calls, emails, and data entry to compile. Many thanks to Janet & Binky for their pioneering work in supplying nutrient data for cat owners. However, re-posting or republishing this chart on any other public platform or website is expressly forbidden. Autoim m unereaction Autoim m unereaction Asym ptom atic and E videnceof autoim m une R eversibleautoim m une Autoim m unereactionwith D eath serologic orother reactioninvolving anonreactioninvolving function life-threatening evidenceof autoim m une essentialorganor of am ajororganorother consequences reaction,with norm al function. F orchildrenandadolescents(fi18yearsof age)withoutabaselinetest,pre-ex posure/pretreatm enthearing shouldbeconsideredtobe<5dBloss. Hypertension Hypertension Asym ptom atic,transient R ecurrentorpersistent R equiring m orethanone L ife-threatening D eath (<24hrs)increaseby>20 (fi24hrs)orsym ptom atic drug orm oreintensive consequences. Adrenalinsufficiencym ustbeconfirm edbylaboratorystudies(low cortisolfrequently accom paniedbylow aldosterone). Anorex ia Anorex ia L ossof appetitewithout O ralintakealtered Associatedwith L ife-threatening D eath alterationineating habits withoutsignificantweight significantweightlossor consequences lossorm alnutrition;oral m alnutrition. Colitis Colitis Asym ptom atic,pathologic Abdom inalpain;m ucus Abdom inalpain,fever, L ife-threatening D eath orradiographic findings orbloodinstool changeinbowelhabits consequences. If salivaryflow m easurem entsareusedforinitialassessm ent,subsequentassessm entsm ustusesalivaryflow. D ysphagia D ysphagia Sym ptom atic,abletoeat Sym ptom atic andaltered Sym ptom atic and L ife-threatening D eath (difficultyswallowing) regulardiet eating/swallowing. E nteritis E nteritis Asym ptom atic,pathologic Abdom inalpain;m ucus Abdom inalpain,fever, L ife-threatening D eath (inflam m ationof thesm all orradiographic findings orbloodinstool changeinbowelhabits consequences. E sophagitis E sophagitis Asym ptom atic pathologic, Sym ptom atic;altered Sym ptom atic and L ife-threatening D eath radiographic,or eating/swallowing. Cholecystitis Cholecystitis Asym ptom atic, Sym ptom atic,m edical Interventionalradiology, L ife-threatening D eath radiographic findingsonly interventionindicated endoscopic,oroperative consequences. Pancreatitis Pancreatitis Asym ptom atic,enz ym e Sym ptom atic,m edical Interventionalradiologyor L ife-threatening D eath elevationand/or interventionindicated operativeintervention consequences radiographic findings indicated. Viralhepatitis Viralhepatitis Present;transam inases Transam inases Sym ptom atic liver D ecom pensatedliver D eath andliverfunctionnorm al abnorm al,liverfunction dysfunction;fibrosisby function. E dem a: E dem a:headandneck L ocaliz edtodependent L ocaliz edfacialorneck G eneraliz edfacialor Severewith ulcerationor D eath headandneck areas,nodisabilityor edem awith functional neckedem awith cerebraledem a; functionalim pairm ent im pairm ent functionalim pairm ent tracheotom yorfeeding. Alternatively,directm easurem entof ioniz edcalcium isthedefinitivem ethodtodiagnose m etabolicallyrelevantalterationsinserum calcium. E x ostosis E x ostosis Asym ptom atic Involving m ultiplesites; E x cisionindicated Progressionto D eath painorinterfering with m alignancy(i. F racture F racture Asym ptom atic, Sym ptom atic butnonSym ptom atic and D isabling;am putation D eath radiographic findingsonly displaced;im m obiliz ation displacedoropenwound indicated. L eukoencephalopathy(radiographic findings)doesnotincludelacunas, which areareasthatbecom evoidof neuraltissue. Chylothorax Chylothorax Asym ptom atic Sym ptom atic; O perativeintervention L ife-threatening. O bstruction/stenosisof Airwayobstruction Asym ptom atic obstruction Sym ptom atic. Pneum othorax Pneum othorax Asym ptom atic, Sym ptom atic; Sclerosisand/or L ife-threatening,causing D eath radiographic findingsonly interventionindicated operativeintervention hem odynam ic instability. Itm aybe difficulttodistinguish from pneum onitisthatisgenerallyseenwithin3m onthsof radiationorcom binedm odalitytherapy. Cytokinerelease Cytokinerelease M ildreaction;infusion R equirestherapyor Prolonged(i. Signsandsym ptom susuallydevelop during or shortlyafterdrug infusionandgenerallyresolvecom pletelywithin24hrsof com pletionof infusion. Signs/sym ptom sm ayinclude:Allergic reaction/hypersensitivity(including drug fever);Arthralgia(jointpain);Bronchospasm;Cough;D iz z iness;D yspnea(shortnessof breath);F atigue(asthenia,lethargy,m alaise);Headache;Hypertension;Hypotension;M yalgia (m usclepain);N ausea;Pruritis/itching;R ash/desquam ation;R igors/chills;Sweating (diaphoresis);Tachycardia;Tum orpain(onsetorex acerbationof tum orpainduetotreatm ent); U rticaria(hives,welts,wheals);Vom iting. The syndrom eisusuallym anifestedbyotherwiseunex plainedfever,weightgain,respiratorydistress,pulm onaryinfiltratesand/orpleuraleffusion,with orwithoutleukocytosis. The sym ptom s/signsincludetum orpain,inflam m ationof visibletum or,hypercalcem ia,diffusebonepain,andotherelectrolytedisturbances. Oyewole 1 Department of Veterinary Physiology, Biochemistry and Pharmacology, University of Ibadan, Ibadan, Oyo state, Nigeria. Accepted 12 February, 2010 Minerals are inorganic nutrients, usually required in small amounts from less than 1 to 2500 mg per day, depending on the mineral. As with vitamins and other essential food nutrients, mineral requirements vary with animal species. For example, humans and other vertebrates need large amounts of calcium for construction and maintenance of bone and normal function of nerves and muscles. Red blood cells can not function properly without iron in haemoglobin, the oxygen-carrying pigment of red blood cells. Iron is also an important component of the cytochromes that function in cellular respiration. Magnesium, copper, selenium, zinc, iron, manganese and molybdenum are important co-factors found in the structure of certain enzymes and are indispensable in numerous biochemical pathways. Sodium, potassium and chlorine are important in the maintenance of osmotic balance between cells and the interstitial fluid. The interactions between nutrition and diseases, nutrition and drug metabolism have been reported. Excessive intake of some minerals can upset homeostatic balance and cause toxic side effects. For example, excess sodium intake is associated with high blood pressure and excess iron can cause liver damage. Also, severe shortages or self-prescribed minerals can alter the delicate balance in body functions that promotes health. The aim of this paper is to review the biochemical functions and the importance of the mineral elements in health and disease conditions of humans, animals and plants as this will assist in the prevention of nutrition-related diseases and maintenance of good health for humans and animals that depend on plants for food. This paper could also serve as a ready source of literature review for researchers involved in nutritional sciences. Although they yield no energy, they have important roles to play in many activities in the body (Malhotra, 1998; Eruvbetine, 2003). Minerals may of minerals to health and this would subsequently assist in be broadly classified as macro (major) or micro (trace) prevention and management of mineral-associated elements. Data on mineral contents of human the macro-minerals include calcium, phosphorus, foods and animal feeds are essential for formulation of sodium and chloride, while the micro-elements include feeding regimes and food processing techniques. The ultra trace elements and plant nutrition has been well recognized (Underwood, include boron, silicon, arsenic and nickel which have 1971; Darby, 1976). Deficiencies or disturbances in the been found in animals and are believed to be essential nutrition of an animal cause a variety of diseases and can for these animals. When a trace essentialness of others like cadmium, lead, tin, lithium element is deficient, a characteristic syndrome is proand vanadium is weak (Albion Research Notes, 1996). The trace elements are other essential nutrients like proteins, fats, carbohyessential components of enzyme systems. Animal husbandry had demonconditioned deficiencies of mineral elements therefore strated the need for minerals in the diet (Hegsted et al.
Buy cheap norpace on line. ANXIETY SIGNS SYMPTOMS AND SOLUTION.
References
- Bodamer O. Creatine metabolism and CblC. OAA Newsletter 2002;12:11.
- Li ZS, Pham TD, Tamir H, Chen JJ, Gershon MD. Enteric dopaminergic neurons: Definition, developmental lineage, and effects of extrinsic denervation. J Neurosci. 2004;24(6):1330-1339.
- Keith SW, Redden DT, Katzmarzyk PT, et al. Putative contributors to the secular increase in obesity: exploring the roads less traveled. Int J Obesity 2006;30(11):1585-94.
- Saran FH, Baumert BG, Khoo VS, et al. Stereotactically guided conformal radiotherapy for progressive low-grade gliomas of childhood. Int J Radiat Oncol Biol Phys 2002; 53(1):43-51.