
Joel C. Rosenfeld MD, MEd, FACS
- Associate Clinical Professor of Surgery, University of Pennsylvania School of
- Medicine, Philadelphia, Pennsylvania
- St. Luke? Hospital and Health Network,
- Bethlehem, Pennsylvania
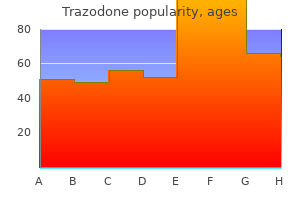
This central clock distributes the message to the rest of the body medicine bag discount trazodone 100mg on-line, in order to synchronise all of its biological functions with the day/night cycle medicine 1950 purchase genuine trazodone on-line. The central biological clock determines the production of a hormone medications metabolized by cyp2d6 order trazodone 100mg online, called melatonin medications going generic in 2016 order genuine trazodone, whose secretion begins in the evening medications kidney disease generic trazodone 100 mg with amex, around two hours before bedtime medications harmful to kidneys cheap 100mg trazodone otc, and then reaches a peak towards the middle of the night before returning to very low and even undetectable levels in the morning and for the rest of the day. The effective synchronisation of the central circadian clock, and thus of the biological functions that depend on it, in particular wake/sleep rhythms, requires high light intensity during the day and total darkness at night. There have been many different publications studying the disruption of circadian rhythms related to exposure to light in the evening or at night. The results of several experimental studies conducted in humans, during which people were subjected to blue-rich light from artificial lighting or screens (computers, telephones, tablets, etc. However, a value of around 10-40 lux or lower (a very low level that can be largely exceeded with domestic lighting) is sufficient to observe an impact on the circadian clock (illustrated by the suppression of nocturnal melatonin secretion). In conclusion, in light of the sufficient evidence provided by studies undertaken in humans, circadian rhythm disruption induced by exposure to blue-rich light during the evening or at night is considered as proven. Furthermore, experimental studies in animals have demonstrated that circulating melatonin in a mother crosses the placental barrier and enters the foetal circulation, which possesses melatonin receptors. Thus, maternal melatonin can impact foetal development, in particular the establishment of the circadian system. At night, maternal exposure to light modifies melatonin levels and induces a prenatal effect that appears to have consequences lasting into adulthood (effects on circadian rhythms, metabolic effects, etc. It can reasonably be assumed that in humans, the effects of modern lighting at night on maternal melatonin secretion negatively impact in utero foetal development. The disruption of circadian rhythms is also associated with other health effects13 (disruption of sleep quality and quantity, metabolic disorders, increased risk of cancer especially breast cancer, cardiovascular diseases, effects on mental health). However, the direct connection between exposure to blue-rich light in the evening or at night and the occurrence of these health effects, while strongly suspected, has not been proven to date in humans. The evidence provided by studies undertaken in humans is sufficient to conclude that exposure to blue-rich light during the evening has a proven effect on sleep onset latency and the duration and quality of sleep. A number of studies have focused on the effects of lighting, especially blue light, on the performance of night workers. The objective has been the short-term optimisation of vigilance and the reduction of sleepiness in order to reduce industrial and traffic accidents and enhance performance and productivity. However, the issue of potential health effects, due to a possible increase in the phototoxicity of light at night, has yet to be defined. Regarding human exposure to blue light in the melanopic band, no data were identified in the scientific literature. An obvious factor is the higher lens clarity of young people, causing more light to pass through than for adults. Exposure to intense and acute light is phototoxic since it causes the irreversible loss of retinal cells, which can lead to partial and permanent (scotoma15, decrease in visual field, reduced resolution) or total (blindness) vision loss. Some experimental studies, currently limited to animals, have demonstrated increased retinal vulnerability to phototoxicity at night, due to a daily photosensitivity rhythm and disruptive effects on the endogenous retinal clock. Furthermore, the review of the scientific literature on myopia and Sjogren syndrome18 led to the following conclusions: the effect of blue-rich light on myopia is possible (whether positive or negative); the effect of blue-rich light on the occurrence of Sjogren syndrome is possible. This syndrome is characterised by ocular discomfort with tingling sensations or an impression of a foreign body in the eye. Adding artificial lighting to natural lighting is likely to modify the ocular doses received by the cornea and retina in the phototoxic band (up to a 50% increase). Indeed, the photons of blue light have higher energy than the photons associated with longer wavelengths. They can therefore induce photochemical reactions similar to those caused by ultraviolet radiation. High energy levels in blue light can therefore be received by the retina without creating a strong visual sensation. Since this blue-coloured light does not necessarily create glare, it can be stared at over a long period, especially by children. It should be noted that lighting devices belonging to risk group 2 (hand-held lamps, head torches, toys and certain vehicle lights) are available on the market. The risk of ocular diseases occurring in relation to exposure to these devices is higher, especially for susceptible population groups. However, the spectral composition of light does not modify the disability glare phenomenon. All studies have consistently shown that (1) non-uniform sources produce more glare than uniform sources, even with moderate luminance, and (2) the higher the contrast, the greater the sensation of discomfort. Moreover, since the scattering of light in ocular environments increases with age, discomfort also increases. However, at the same colour temperature, the spectral composition and especially the blue-light enrichment of the spectrum has probable consequences on visual discomfort. Furthermore, there is a high level of inter-individual variability in the general population as to the assessment of glare situations. Deterioration of vision accelerates after the age of 60, at varying rates depending on the individual. The stray light generated around sources increases considerably with age, lowering the perception of object contrast and therefore visual performance. Subjects with migraine seem to be specifically susceptible to the glare caused by certain irregularities in the spectral distribution of light energy. The experts conclude that the effect of exposure to blue-rich light on the occurrence of skin diseases is possible. Of the five studies undertaken to assess the risk of developing benign or malignant melanocytic lesions following blue-light neonatal phototherapy, three showed an increased number of common or atypical naevi in exposed children. Depending on its frequency, this modulation may or may not be perceptible by the human visual system. Three separate visual effects (conscious perception of modulation) have been described: flicker, the stroboscopic effect and the phantom array effect. The health effects that can result from the conscious or unconscious perception of modulation are epilepsy attacks, traffic accidents, accidents related to the use of machines, migraines, headaches and visual fatigue. Effects such as headaches, migraines and visual fatigue can be associated with temporal modulation frequencies between 80 and 120 Hz. Phenomena such as the stroboscopic effect (apparent immobility or slowing of a moving object) and the phantom array effect (persistence of an image during a visual saccade) can occur at high modulation frequencies (greater than around 80 Hz). In an industrial or domestic context, it is likely that the stroboscopic effect could affect safety during the use of machines or tools. Temporal light modulation can also be associated with the triggering of attacks in people with epilepsy. At certain speeds, the temporal modulations are located around 15 Hz, in the most critical band for the triggering of epilepsy attacks. In all of these situations, temporal light modulation is associated with visual discomfort and a decrease in visual efficiency, especially at workstations in occupational settings. Epidemiological studies showing an association between modulated light and the triggering of migraine refer to migraine patients as a population group sensitive to modulated light. Work undertaken using older-generation fluorescent tubes showed that certain individuals had heightened sensitivity to temporal light modulations at the frequency of 100 Hz. In addition, studies have shown that some individuals visually perceive flicker at 100 Hz. Thus, with regard to certain health effects related to temporal light modulation, several susceptible population groups were identified: regarding headaches, migraine and visual fatigue: children, adolescents and young adults; migraine sufferers; regarding the risk of accidents related to the stroboscopic effect or phantom array effect: machine and tool operators and vehicle drivers; people with motor or cognitive disorders reducing their avoidance or decision-making capacities; children, adolescents and young adults; regarding the triggering of epilepsy attacks: people with epilepsy. According to the measurements taken for this expert appraisal: specific blue-light-blocking glasses were more effective at filtering than treated ophthalmic lenses. It cannot be said that this filtration is sufficient to prevent the decrease in melatonin secretion induced by exposure to light in the evening and the related effects of sleep onset delay; for the tested screens claiming to limit blue-light emissions, no real effectiveness was observed. However, reducing the colour temperature (switching to warm white) and brightness of the screens was somewhat effective at reducing the quantity of blue light in the spectrum. Thus, what might be an advantage for a given plant or animal species may prove to be a disadvantage for another. Changes in the (daily and annual) biological rhythms, orientation, geographical distribution and migration of species can thus be observed following exposure to artificial light. There can also be indirect effects (in the medium and long term) on these populations and their ecosystems. These effects are combined with other anthropogenic pressures (chemical pollution, geographical barriers, shrinking habitats, overexploitation, etc. The continuous extension of human, industrial and leisure activities in addition to physical and chemical nuisances combined with the effects of climate change are all factors that certain animal and plant populations will probably be incapable of coping with, which will speed up the decline in biodiversity. However, data involving the combined action of these multiple disruptive factors are still extremely scarce. Various aspects have been considered, such as effects on the sky glow, nuisances for humans (intrusive light, light trespass, glare, circadian rhythms) and nuisances for ecosystems and biodiversity. In these categories, the trend is towards an increase in the number and intensity of points of light. This recommendation will limit the visibility of the phantom array effect, which is a source of proven visual disturbances; introducing the option to automatically lower the colour temperature (switch to warm white) and brightness of mobile telephone and tablet screens before bedtime. Light is modulated at a fixed frequency and the change in the duty cycle modifies the average light intensity. Since potentially beneficial effects of a strong light contrast between daytime and night-time have been described in the scientific literature, it will be necessary to: confirm the effects of exposure to sufficient daytime light intensities on quality of life, sleep, well-being and health, especially for people with circadian rhythm disorders (elderly subjects, hospitalised patients, people with dementia, etc. Special attention should be paid to certain susceptible population groups (children, adolescents, people with ocular diseases, aphakic individuals, etc. It would also be advisable to study to what extent phototoxicity results obtained in rodents can be extrapolated to humans. In particular, it recommends conducting: studies to better identify inter-individual variations in sensitivity to temporal contrasts and better understand the prevalence and incidence of effects related to temporal light modulation in the general population; studies enabling the risk of accidents arising from exposure to a stroboscopic effect or phantom array effect to be quantified. To do so, it used a methodology for assessing the levels of evidence associated with the health effects in question. The new scientific data examined corroborated the findings of 2010 relating to phototoxicity and enabled the experts to establish that the retinal phototoxicity of acute exposure to blue-rich light is proven. Children and adolescents, exposed from a very early age to screens in particular (tablets, game consoles, mobile telephones, etc. Although the health risks associated with exposure to this modulation have not been determined, some people (children, adolescents, young adults, machine operators and vehicle drivers, etc. It encourages the establishment of standards defining performance criteria for personal protective equipment in relation to blue light. The Agency thus underlines the need to enforce the current regulations and adapt them, in particular by limiting the number of points of light and reducing light pollution, all while taking care to ensure the safety of people. The specific goals of the present study were to: (1) perform photometric measurements at workstations in winter and late spring, and (2) analyze the impacts of personal light exposure on circadian entrainment using a wearable light and activity measurement device. Reported here are the results of the measurements performed during two seasons in a building located in the Northwest region of the United States. Keywords: Light, Daylight, Building Design, Circadian Light, Sleep, Mood 1 Background It is well known that people like daylight in their work environment (Boyce et al. It has been argued that daylight also positively affects performance (Heschong Mahone Group, 1999; 2003a; b). Daylight is certainly not a special light source for vision, and the link between improved performance cannot be reliably shown (Boyce, 2004; Boyce and Rea, 2001). Another line of research based upon human circadian system response to light may provide insight into the widely accepted, but again undocumented belief that daylight improves productivity as well as health and wellbeing. Basic research in circadian photobiology (Arendt, 1995; Klein, 1993; Moore, 1997; Turek and Zee, 1999) suggests that light plays a very important role in regulating the daily patterns of human behaviour by directly affecting the internal timing mechanisms of the body (Jewett et al. Examples of circadian rhythms include the daily variations in behavior, like the sleep-wake cycle, hormone production, and core body temperature. In the absence of external cues, circadian rhythms in humans will run with a period close to , but not exactly 24 hours (in humans, circadian rhythms free run with a period of 24. The light-dark patterns on the retina are the main stimuli driving the biological clock to synchronize circadian rhythms to the 24-hour day. Important light characteristics affecting the human circadian system include the spectral power distribution of the light source (amount and spectrum), timing and duration of exposure, spatial distribution, and light history. In terms of temporal characteristics, operation of the visual system does not depend significantly on the timing of light exposure, and thus responds well to a light stimulus at any time of the day or night. Figures 1 and 2 show spectral and absolute sensitivities of the human circadian system based on the proposed model by Rea et al. Left: A selection of spectral sensitivity functions for the human visual and circadian systems. The photopic luminous efficiency function, V, with a peak at 555 nm is shown in black and is a good approximation of the spectral sensitivity of the human fovea for such achromatic tasks such as reading and acuity (Lennie et al. Three non-linear spectral sensitivity functions for the human circadian system at one light level; each function reflects differences in sensitivity of the human circadian system to different light spectra. The dashed line represents the sensitivity of the human circadian system to individual, narrow band light spectra as measured in terms of nocturnal melatonin suppression (Brainard et al. Circadian stimulus is proportional to nocturnal melatonin suppression; values range from 0 at or below threshold to 0.
As a result medicine of the wolf buy generic trazodone 100mg on-line, crewmembers obtained relatively good sleep on the West Coast layovers and did not need additional days to readapt to West Coast time at the end of the trip medicine yeast infection purchase cheap trazodone. On the other hand medications used to treat anxiety discount 100mg trazodone visa, when they arrive back in their home time zone medicine 7 years nigeria order trazodone online, they need additional days to readapt to local time medicine evolution purchase trazodone from india. The scarcity of data on what happens to the circadian body clock across different long haul trip patterns is one reason most current bio-mathematical models do not have a validated approach for simulating what happens to the circadian clock across sequences of trans-meridian flights (see Chapter Four) medications containing sulfa purchase trazodone visa. The science does not address every detailed operational question and it never will. Unrestricted sleep means being free to fall asleep when tired and wake up spontaneously, with sleep occurring at the appropriate time in the cycle of the circadian body clock. In some cases, this recovery period can be built into schedules (for example with short day time duty periods). It is a valuable personal mitigation strategy, for example prior to a night duty period or on long haul flights. The homeostatic sleep process is evident in the pressure for slow-wave sleep that builds up across waking and discharges across sleep. Its sensitivity to light enables it to stay in step with the 24-hour day/night cycle. On return to the home time zone, additional days are needed to readapt to local time. On the other hand, on return to the home time zone, additional days are needed to readapt to local time. Does the sleep opportunity occur at an appropriate time in the circadian body clock cycle. From a safety perspective, the answer is that no single defensive strategy is 100% sure. For example, there is a tendency to believe that an operation is safe if it is predicted to be below the threshold, but unsafe if it is predicted to be above it. Maintaining the required documentation is one of the recommended functions of the Fatigue Safety Action Group Figure 3. All other operations will be conducted under the prescriptive flight and duty time regulations. Management is primarily responsible for the management of fatigue risk because it controls the activities of personnel and the distribution of resources in the 16 organization. For example, crewmembers have personal responsibility because they can choose the amount of time they spend trying to sleep during available rest breaks, and choose when to use personal fatigue mitigation strategies (Chapter Four). All other operations will operate under the prescriptive flight and duty time regulations. Fatigue Risk Management must be considered a core part of our business as it provides a significant opportunity to improve the safety and efficiency of our operation and to maximise the well being of our staff. These challenges require our flight crews to perform at the highest levels of competence and professionalism at all times. We need to manage these risks carefully in order to make consistently sound decisions, particularly to balance the critical needs of patients with the requirement for safe operations. This can only be achieved through the shared responsibility and commitment of management, crew members (pilots, doctors and nurses) and our support staff. Chief Pilot, Operations Manager) who are not part of your crew are used to support crew decision making. The effective management of fatigue is critical to ensuring that our company can deliver a quality service to our customers. However, it needs to be accessible to all personnel who may need to consult it, and to the regulator for audit. As a way of meeting these requirements, it is recommended that an operator create a functional group that is responsible for coordinating the fatigue management activities within the organisation. The composition of the Fatigue Safety Action Group should reflect the shared responsibility of individuals and management by including representatives of all stakeholder groups (management, scheduling staff, and crewmember representatives) and other individuals as needed to ensure that it has appropriate access to scientific and medical expertise. In small operators, a single individual may represent more than one stakeholder group, for example the chief pilot may also be the primary scheduler. In very small operators, there may not even be a designated Fatigue Safety Action Group, simply extra items on the Safety Meetings agenda, as long as long as all fatigue risk management activities are documented. Larger airlines will have specialized departments that interact with the Fatigue Safety Action Group. As an initial step, the Fatigue Safety Action Group, or other appropriate entity within the organisation, will need to identify through a risk assessment process, differences between scheduled and actual flight times, duty periods and rest periods that will be considered significant within the context of their specific operations. Further, the Fatigue Safety Action Group will also be responsible for establishing a process for monitoring such significant deviations and documenting any subsequent actions taken. Such definitions will need to be provided to the regulator for their acceptance and it will be important that there is a clear understanding between the regulator and the operator as to what constitutes a significant deviation. The regulator may also use these to identify criteria for when the operator must notify them immediately. This includes responsibility for gathering, analyzing, and reporting on data that facilitates the assessment of fatigue-related risk among flight crewmembers. Its membership will include at least one representative of each of the following groups: management, scheduling, and crewmembers, with other specialists as required. Minutes will be taken during meetings and distributed within 10 working days after each meeting. Identification of hazards An operator shall develop and maintain three fundamental and documented processes for fatigue hazard identification: 2. Predictive the predictive process shall identify fatigue hazards by examining crew scheduling and taking into account factors known to affect sleep and fatigue and their effects on performance. Methods of examination may include but are not limited to: a) operator or industry operational experience and data collected on similar types of operations; b) evidence-based scheduling practices; and c) bio-mathematical models 2. Proactive the proactive process shall identify fatigue hazards within current flight operations. Methods of examination may include but are not limited to: a) self-reporting of fatigue risks; b) crew fatigue surveys; c) relevant flight and cabin crew performance data; d) available safety databases and scientific studies; and e) analysis of planned versus actual time worked 2. Reactive the reactive process shall identify the contribution of fatigue hazards to reports and events associated with potential negative safety consequences in order to determine how the impact of fatigue could have been minimized. Risk assessment An operator shall develop and implement risk assessment procedures that determine the probability and potential severity of fatigue-related events and identify when the associated risks require mitigation. The risk assessment procedures shall review identified hazards and link them to: a) operational processes; b) their probability; c) possible consequences; and d) the effectiveness of existing safety barriers and controls. Collect and analyze data and use available information on potential fatigue hazards. Decide which risks require mitigation Implement appropriate mitigation strategies and 5a. Set safety performance whether the mitigation strategies are delivering the indicators required level of risk reduction. If mitigation strategies perform to an acceptable standard, they become part of normal operations and are monitored 6. Further, as described in Chapter 2, different types of flight operations can involve different causes of crewmember fatigue and may require different controls and mitigation strategies to mitigate the associated risks. To do this, the group needs to have a good understanding of the operational factors that are likely to cause crewmember fatigue. The domestic night cargo operations (2 pilots, 1 flight engineer) had the shortest duty periods, averaged 3 flights per duty period, and had longer rest periods than the short haul operations. The long haul operations (2 pilots, 1 flight engineer) had long duty periods, but averaged only 1 flight per duty period and had the longest rest periods. However, every layover was in a different time zone, with a maximum of 8 time zones crossed per 24 hours. As a result, additional time for circadian re-adaptation was needed for full recovery after the trip. Unscheduled operations pose particular challenges, because it is hard to plan sleep when you do not know when you have to work, or for how long. It may be possible to identify potential fatigue hazards based on information and operational experience from similar types of operations flown by the operator or other carriers, or from published scientific studies of fatigue in similar operations. In addition, the Fatigue Safety Action Group may sometimes decide to undertake non-routine data collection to better understand specific fatigue hazards (for example, a one-off fatigue survey at a crew base, or a targeted monitoring study on a route where fatigue is identified as a concern). Different types of information and data that can be collected are described in the following sections and in Appendix B. As already mentioned, various types of data are involved including measures of operational performance, which operators are familiar with, and measures of the fatigue levels of crewmembers, which will be less familiar to most operators. The following sections and Appendix B provide guidance about measuring crewmember fatigue. On some occasions, it may be appropriate for the Fatigue Safety Action Group to seek external scientific advice in this area. However, it is also possible for an operator to develop in-house expertise in fatigue data collection and analysis. The complexity of operations and the level of fatigue risk need to be considered evaluating the need for, and level of, expert advice. For example, crewmembers may recognize a particular destination within a proposed schedule as generating a high level of fatigue because of their past experience of regular delays there caused by heavy traffic. Schedulers may know that a particular city pairing regularly exceeds planned flying time. Management may organize for crew to stay in another hotel where noise is a known problem. For existing operations, information about schedules may already be available that could be analyzed to check for potential fatigue hazards. When operational demands are changing, reliance on previous experience can have some limitations. Scheduling based only on previous experience may not give the most robust or innovative solutions for new situations. It may also be important to collect data on actual levels of crew fatigue, to check whether the lessons from previous experience are still valid in the new context. Another way to identify fatigue hazards related to scheduling, for existing or new routes, is to look for information on similar routes. This could include incident reports and crew fatigue reports, or published scientific research and other information available on similar routes flown by other operators. This means considering factors such as the dynamics of sleep loss and recovery, the circadian biological clock, and the impact of workload on fatigue, along with operational requirements. Since the effects of sleep loss and fatigue are cumulative, evidence-based scheduling needs to address both individual trips (multiple, successive duty periods without extended time off), and successive trips across rosters or monthly bid-lines. The following are examples of general scheduling principles based on fatigue science. It does adapt progressively to a new time zone, but full adaptation usually takes longer than the 24-48 hours of most layovers.
Constraints on communication parties symptoms 5-6 weeks pregnant buy trazodone with amex, which hinder their ability to meet this goal medications 126 buy cheap trazodone on-line, must be recognised and overcome pretreatment buy trazodone 100 mg on-line. Every country needs a system with independent expertise to ensure that safety information on all available drugs is adequately collected medications you can give your cat order generic trazodone line, impartially evaluated symptoms prostate cancer generic 100 mg trazodone otc, and made accessible to all treatment yeast infection women buy trazodone 100mg line. Exchange of data and evaluations among countries must be encouraged and supported. A strong basis for drug safety monitoring has been laid over a long period, although sometimes in response to disasters. Innovation in this field now needs to ensure that emergent problems are promptly recognised and efficiently dealt with, and that information and solutions are effectively communicated. These ideals are achievable and the participants at the conference commit themselves accordingly. Details of what might be done to give effect to this declaration have been considered at the conference and form the substance of the conference report. Throughout the various meetings, concepts were presented and debated, drafts of proposals were reviewed and discussed, and two surveys of the industry were carried out (one on practices and experience in preparing periodic safety update reports (see Chapter 4) and the other on knowledge and use of patient exposure information (see Chapter 5)). The meetings subsequent to April 1997 were as follows: July 1997 (Geneva), November 1997 (New York), April 1998 (Paris), November 1998 (Philadelphia), March 1999 (Amsterdam), July 1999 (Berlin), and August 2000 (Barcelona). In May 1999 and February 2000, the appointed editorial committee for the report (A. Lumpkin) held meetings to resolve outstanding issues and design the overall report. However, it is common practice to rely on at least two such sources for literature searches. Perhaps the two most widely used general biomedical databases for this purpose are Medline and Embase. In addition there are several more general biological and scientific databases such as SciSearch, Biosis, and the Derwent Drug File. There are also specialized databases which deal with specific disease areas (such as CancerLit and AidsLine), or with the toxicological effects of drugs (ToxLine). Medline Medline is a vast source of medical information, covering the whole field of medicine including dentistry, veterinary medicine and medical psychology. The database covers clinical medicine, anatomy, pharmacol ogy, toxicology, genetics, microbiology, pathology, environmental health, occupational medicine, psychology, and biomedical technology, etc. The database corresponds to the printed publications: Index Medicus, Index to Dental Literature, International Nursing Index and various biblio graphies. It is also available in many manifestations on the World Wide Web, several of which are free to use. It features unique international journal coverage and includes many important journals from Europe and Asia not found in other biomedical database; overall coverage is approximately 4,000 journals published in 70 countries. The emphasis of the database is on the pharmacological effects of drugs and chemicals. Additional areas of coverage are human medicine and biological sciences relevant to human medicine, health affairs (occupational and environmental health, health economics, policy and management), drug and alcohol dependence, psychiatry, forensic science, pollution control, biotechnology, medical devices and alternative medicine. It indexes all significant items (articles, review papers, meeting abstracts, letters, editorials, book reviews, correction notices, etc. Some 3,800 of these journals are further indexed by the references cited within each article, allowing for citation searching. It selectively covers the worldwide pharmaceutical literature; papers chosen may cover the chemistry, analysis, pharmaceutics, pharmacology, metabolism, biochemistry, interactions, therapeutic effects and toxicity of a drug. Papers from over 1,150 scientific and medical journals and conference proceedings are included. Each year approxi mately 9,000 articles on adverse drug reactions are published in the scientific literature. All articles are sent to recognised authorities who critically assess the information and distil the key elements for inclusion. Speculative or unsubstantiated statements on the side effects of ethical drugs are not included. The database consists of bibliographic records referencing cancer research publications dating from 1963 to the present. In addition, proceedings of meetings, government reports, symposia reports, selected monographs, and theses are also abstracted for inclusion in the database. Even with a single company statement, however, there can well be debate and sometimes discrepant views between personnel within an organization as to what a safety data mean. In addition, 22 physician monitors enployed by either Glaxo or SmithKline Beecham Pharmaceuticals completed the exercise. Despite these efforts, reporting discrepancies within and between organisations are ocurring. These are felt to be not only due to cultural differences between organizations and regulatory agencies. In the absence of standardized guidelines, such opinions caused by a nonstandar dized view can lead to the same case history being reported to some regulatory authorities but not to others, even though reporting is based on the same reference data and similar regulations. No attempt was made to compare responses from regulators attending the meeting with the others, although it would have been interesting. As can be seen, there appears to be a different philosophy between Europe and the United States in the way the events are interpreted, particularly where the outcome is death (examples 6 and 9). Individuals in the United States would tend to report a fatality as an unlabeled event, whereas in Europe this is generally viewed as an outcome rather than a factor relevant to labeledness. For example, in Europe, 97% of the respondents accept that if myocardial infarction is to be labeled, death 230 due to myocardial infarction is also labeled. Only 43% of the respondents in the United States, however, would accept fatal myocardial infarction to be labeled if only myocardial infarction appeared in the labeling. Also of interest is that in Europe, rather than the United States, cyanosis secondary to hypoventilation was equated with respiratory depression (Example 8). As can be seen, medical opinion was unanimous among 22 medical monitors in only one example (Example 1) where the greater anatomical specificity did not affect the labeledness of lung fibrosis. Table 2 was designed to gather responses on whether certain medical events should be considered to be serious. For instance, in Example 1, total blindness for 30 minutes was considered to be serious in Europe, whereas in Example 3, mild anaphylaxis was thought to be serious in the United States. This is in contrast to the overall total of 95% who consider this event to be serious. The information found in Table 3 was designed to determine whether the respondents felt, based on the available case details, the case should be reported to regulatory authorities. The results suggest a fairly uniform transatlantic view about whether or not a case should be reported. Fewer in Europe than in the United States, however, would report a case where the reporter could not remember the age or even the sex of a patient (Example 167). Discussion None of the 30 examples surveyed achieved a totally unanimous view and so the guidelines presented below are all based on a majority verdict. To some extent the non-uniform opinion is surprising because of the relatively small number of individuals who took part in the survey, with many having a substantial amount of expertise in the area of drug safety. It appears that in many situations reporting is practiced according to medical common sense. It is believed that the newly proposed United States regulations, in the wake of fialuridine experience, should serve to move general opintion further toward reporting based on medical opinion. Worthy of comment is that the extra reporting is not always within the United States. For example, blindness for 30 minutes, respiratory collapse, and respiratory depression would be more frequently viewed as medically serious and would be reported more often in Europe. The United States reporting practice is more to view fatalities as unlabeled unless death is specifically mentioned in the label. Before suggesting a pragmatic way forward to best benefit from the harmonization initiatives, the following 20 guidelines are proposed. An unlabeled diagnosis which relates to a group of symptoms or signs which are labeled, the new case is not in itself labeled. For example, if anaphylaxis is labeled, then a report of a patient who experienced hypotension, wheezing, and urticaria would be considered to be labeled (69%). If a report is serious in the medical sense, even though it is not serious in the regulatory sense. On the other hand, a threat of suicide is not considered to be serious (83%), nor in itself is an emergency room or outpatient department visit (97%). If the investigator persists in specifying a case is drug-related, even though this view is medically nonsensical, the case should be considered drug-related and reported to the regulatory authorities. Spontaneously reported cases should always be considered to be possibly drug-related, even if an alternative explanation is given by the reporter (72%). The overall majority of individuals surveyed would not report to regulatory authorities a case where the details of a specific patient could not be recalled. In the United States, however, 72% would report the unidentified patient and 59% the series of eight cases. In those instances where the brand name of a generic drug is stated to be unknown, the case should be processed and reported to regulatory authorities by the company which becomes aware of the adverse event (70%). In the United States, this obligation generally falls to the original brand name manufacturer of the drug. Even with a single company statement, however, there is often debate and sometimes discrepant views between personnel within the organization. Such a nonstandardized company view can lead to the same adverse event case report being reported to some authorities and not reported to others elsewhere, even when judged against the same source reference document. Regulators, partly due to their position, seem to be more pragmatic in their views (previously cited example regarding spontaneous abortion). Often the problem is within the company itself where sometimes (particularly in the United States) there is a need to adhere to a legalistic interpretation of the regulations. If one accepts the last guideline, that if in doubt report, and bears in mind that the core safety data sheet contains the central elements pertinent to safe use of the drug, wherever in the world the drug is marketed, it should be easy to determine the company stance for labeledness equivalence, and the company can then generate a universal list of adverse events which would always be viewed as medically, and consequently regulatory, serious by that organization. Difficulties often emerge in the case evaluation process, particularly in the absence of clear criteria such as hospitalization, life-threatening, death; in such cases, medical judgement is called for. Such a list is not meant to be a substitute for case-by-case review and decisionmaking; however, it can provide a mechanism for assigning medical seriousness in the absence of detailed and confirming information. As a result, the sample list presented should not be regarded as thorough or definitive, but rather a starting point. Different users may wish to develop their own custom-designed list to serve their special needs related to the medical aspects of their products and the diseases they treat. The terms given do not necessarily refer to a serious condition per se, but may be indicative of a serious syndrome. Paragraph numbering is also used for demonstration purposes to highlight the order proposed for the template. Case reference number 16041938 is a spontaneous case report sent by a hospital pharmacist which refers to a male aged 84 years. The following drugs are known to have been taken by the patient prior to the event (start date in parentheses): cimetidine (1996), steroids (1990) and tetracycline (September 9, 1999).
Generic trazodone 100 mg on line. Streptococcus Beta-hemolytic.
References
- Gayowski T, Marino IR, Singh N, et al. Orthotopic liver transplantation in high-risk patients: risk factors associated with mortality and infectious morbidity. Transplantation. 1998;65(4): 499-504.
- Harzer K, Sandhoff K, Schall H, Kollman F. Enzymatische untersuchungen im blut von ubertragern einer variante der Tay-Sach's schen erkrankung (variante O). Klin Wschr 1971;49:1189.
- Palta S, Gill KS, Pai RG: Role of inadequate adaptive left ventricular hypertrophy in the genesis of mitral regurgitation in patients with severe aortic stenosis: Implications for its prevention, J Heart Valve Dis 12:601, 2003.
- Pressman D, Rolnick D, Turbow B: Penile horn, Am J Surg 104:640n641, 1962.
- Ra-domised trial compari-g tacrolimus (FK506) a-d cyclospori- i- preve-tio- of liver allograft rejectio-. Europea- FK506 Multice-tre Liver Study Group. La-cet. 1994;344(8920):423-428.
- Jolliet P, Chevrolet JC. Bronchoscopy in the intensive care unit. Intensive Care Med. 1992;18:160-169.