
Richard P Gerraty MD, FRACP
- Neurologist, The Alfred Hospital, Melbourne, Vic
- Associate Professor, Department of Medicine, Monash University
Transition may or may not include feminization or masculinization of the body through hormones or other medical procedures gastritis juice fast phenazopyridine 200 mg line. These reviews can serve as detailed references for providers chronic gastritis metaplasia purchase 200 mg phenazopyridine with amex, along with other widely recognized gastritis biopsy order generic phenazopyridine from india, published clinical materials gastritis video cheap phenazopyridine 200mg free shipping. World Professional Association for Transgender Health 99 the Standards of Care 7th Version other side efects of feminizing therapy: the following effects may be considered minor or even desired gastritis symptoms tiredness buy phenazopyridine line, depending on the patient gastritis diet �������� buy cheap phenazopyridine 200 mg line, but are clearly associated with feminizing hormone therapy. However, both spironolac to ne and cyproterone acetate are widely used and deserve some comment. Cyproterone acetate is a progestational compound with anti-androgenic properties (Gooren, 2005; Levy et al. Although widely used in Europe, it is not approved for use in the United States because of concerns about hepa to to xicity (Thole, Manso, Salgueiro, Revuelta, & Hidalgo, 2004). Spironolac to ne is commonly used as an anti-androgen in feminizing hormone therapy, particularly in regions where cyproterone is not approved for use (Dahl et al. Spironolac to ne has a long his to ry of use in treating hypertension and congestive heart failure. However, methyltes to sterone is no longer available in most countries and should no longer be used. World Professional Association for Transgender Health 101 the Standards of Care 7th Version Psychiatric Masculinizing therapy involving tes to sterone or other androgenic steroids may increase the risk of hypomanic, manic, or psychotic symp to ms in patients with underlying psychiatric disorders that include such symp to ms. This adverse event appears to be associated with higher doses or supraphysiologic blood levels of tes to sterone inconclusive or no increased risk: Items in this category include those that may present risk, but for which the evidence is so minimal that no clear conclusion can be reached. There are no data that suggest or show an increase in risk in those with risk fac to rs for dyslipidemia. World Professional Association for Transgender Health 103 the Standards of Care 7th Version Acne, androgenic alopecia Acne and varying degrees of male pattern hair loss (androgenic alopecia) are common side effects of masculinizing hormone therapy. Criteria for Feminizing/Masculinizing Hormone Therapy (one referral or chart documentation of psychosocial assessment) 1. If signifcant medical or mental concerns are present, they must be reasonably well-controlled. If signifcant medical or mental health concerns are present, they must be reasonably well con trolled. Criteria for genital surgery (two referrals) Hysterec to my and ovariec to my in FtM patients and orchiec to my in MtF patients: 1. Persistent, well documented gender dysphoria; World Professional Association for Transgender Health 105 the Standards of Care 7th Version 2. The aim of hormone therapy prior to gonadec to my is primarily to introduce a period of reversible estrogen or tes to sterone suppression, before a patient undergoes irreversible surgical intervention. These criteria do not apply to patients who are having these surgical procedures for medical indications other than gender dysphoria. Me to idioplasty or phalloplasty in FtM patients and vaginoplasty in MtF patients: 1. Although not an explicit criterion, it is recommended that these patients also have regular visits with a mental health or other medical professional. Because of the controversial nature of sex reassignment surgery, this type of analysis has been very important. These changes were not seen as positive; rather, they showed that many individuals who had entered the treatment program were no better off or were worse off in many measures after participation in the program. These fndings resulted in closure of the treatment program at that hospital/medical school (Abramowitz, 1986). Subsequently, a signifcant number of health professionals called for a standard for eligibility for sex reassignment surgery. In 1981, Pauly published results from a large retrospective study of people who underwent sex reassignment surgery. This study included patients who were treated before the publication and use of the Standards of Care. Since the Standards of Care have been in place, there has been a steady increase in patient satisfaction and decrease in dissatisfaction with the outcome of sex reassignment surgery. Studies conducted after 1996 focused on patients who were treated according to the Standards of Care. The fndings of Rehman and colleagues (1999) and Krege and colleagues (2001) are typical of this body of work; none of the patients in these studies regretted having had surgery, and most reported being satisfed with the cosmetic and functional results of the surgery. Quality of surgical results is one of the best predic to rs of the overall outcome of sex reassignment (Lawrence, 2003). The vast majority of follow-up studies have shown an undeniable benefcial effect of sex reassignment surgery on pos to perative outcomes such as subjective well being, cosmesis, and sexual function (De Cuypere et al. A weakness of that study is that it recruited its 384 participants by a general email rather than a systematic approach, and the degree and type of treatment was not recorded. Study participants who were taking tes to sterone had typically being doing so for less than 5 years. Reported quality of life was higher for patients who had undergone breast/chest surgery than for those who had not (p<. Scores were compared to those of 20 healthy female control patients who had undergone abdominal/pelvic surgery in the past. Quality of life scores for transsexual patients were the same or better than those of control patients for some subscales (emotions, sleep, incontinence, symp to m severity, and role limitation), but worse in other domains (general health, physical limitation, and personal limitation). It is diffcult to determine the effectiveness of hormones alone in the relief of gender dysphoria. Most studies evaluating the effectiveness of masculinizing/feminizing hormone therapy on gender dysphoria have been conducted with patients who have also undergone sex reassignment surgery. Favorable effects of therapies that included both hormones and surgery were reported in a comprehensive review of over 2000 patients in 79 studies (mostly observational) conducted between 1961 and 1991 (Eldh, Berg, & Gustafsson, 1997; Gijs & Brewaeys, 2007; Murad et al. Patients operated on after 1986 did better than those before 1986; this refects signifcant improvement in surgical complications (Eldh et al. Most patients have reported improved psychosocial outcomes, ranging between 87% for MtF patients and 97% for FtM patients (Green & Fleming, 1990). Weaknesses of these earlier studies are their retrospective design and use of different criteria to evaluate outcomes. A prospective study conducted in the Netherlands evaluated 325 consecutive adult and adolescent subjects seeking sex reassignment (Smith, Van Goozen, Kuiper, & Cohen-Kettenis, 2005). Patients who underwent sex reassignment therapy (both hormonal and surgical intervention) showed improvements in their mean gender dysphoria scores, measured by the Utrecht Gender Dysphoria Scale. Scores for body dissatisfaction and psychological function also improved in most categories. This is the largest prospective study to affrm the results from retrospective studies that a combination of hormone therapy and surgery improves gender dysphoria and other areas of psychosocial functioning. There is a need for further research on the effects of hormone therapy without surgery, and without the goal of maximum physical feminization or masculinization. In current practice there is a range of identity, role, and physical adaptations that could use additional follow-up or outcome research (Institute of Medicine, 2011). Invited papers were submitted by the following authors: Aaron Devor, Walter Bockting, George Brown, Michael Brownstein, Peggy Cohen-Kettenis, Griet DeCuypere, Petra DeSutter, Jamie Feldman, Lin Fraser, Arlene Istar Lev, Stephen Levine, Walter Meyer, Heino Meyer-Bahlburg, Stan Monstrey, Loren Schechter, Mick van Trotsenburg, Sam Winter, and Ken Zucker. Most were completed by September 2007, with the rest completed by the end of 2007. The fnal papers were published in Volume 11 (1-4) in 2009, making them available for discussion and debate. A subgroup of the Revision Committee was appointed by the Board of Direc to rs to serve as the Writing Group. The Board also appointed an International Advisory Group of transsexual, transgender, and gender nonconforming individuals to give input on the revision. From the survey results, the Writing Group was able to discern where these experts s to od in terms of areas of agreement and areas in need of more discussion and debate. World Professional Association for Transgender Health 109 the Standards of Care 7th Version the Writing Group met on March 4 and 5, 2011 in a face- to -face expert consultation meeting. They reviewed all recommended changes and debated and came to consensus on various controversial areas. These decisions were incorporated in to the draft, and additional sections were written by the Writing Group with the assistance of the technical writer. The draft that emerged from the consultation meeting was then circulated among the Writing Group and fnalized with the help of the technical writer. Discussion was opened up on the Google website and a conference call was held to resolve issues. Feedback from these groups was considered by the Writing Group, who then made further revision. Funding the Standards of Care revision process was made possible through a generous grant from the Tawani Foundation and a gift from an anonymous donor. Process of soliciting international input on proposed changes from gender identity professionals and the transgender community; 3. This Statement may providing this healthfirelated services for all people, including also be useful for 2) primary care providers and people of diverse sexual orientations and gender physicians from any specialty who are interested service may assist identities. For many transgender people, hormone therapy is part of the affrmation of their gender identity, i Available at. Current medical views on For most people, their sense of gender identity is gender identity/transgenderism congruent with their biological sex. For some people, their recognition as being a gender that Transgender people are individuals of any age is different from their assigned sex can happen during whose gender identity and expression does not childhood itself; for others this recognition may arise conform to norms and expectations traditionally during adolescence, or even in early or late adulthood. The World Professional Association of transgender people who do not have intersex for Transgender Health stresses that only some conditions. It includes physical individuals whose gender identity and expression attributes such as sex chromosomes, gonads, sex does not conform to norms and expectations hormones, internal reproductive structures and traditionally associated with their sex assigned at external genitalia. Transgender individuals may selfiidentify as transgender, female, male, trans woman or trans Gender is a term that is often used to refer to man, transsexual, genderqueer, hijra, kathoey, the ways that people act, interact or feel about waria or one of many other transgender identities, themselves, which are associated with boys/men and may express their genders in a variety of and girls/women. Also known as transgender which may or may not correspond with the sex woman or trans woman. It includes both the personal sense of the body, which may involve, if freely Femalefi to fimale transgender person is an individual chosen, modifcation of bodily appearance or who is born as a natal female (female sex by birth) function by medical, surgical, or other means, but whose gender identity is a man (or infibetween and other expressions of gender, including dress, woman and man).
Your doc to r will speak with you about the different types of hormone therapy available and what is best for you gastritis duration of symptoms purchase phenazopyridine 200 mg mastercard, depending on your specifc needs and situation gastritis yeast infection phenazopyridine 200 mg cheap. Tablets to block the effects of tes to sterone (anti-androgens) Anti-androgen drugs s to p tes to sterone from getting to the prostate cancer cells so they are not able to grow gastritis chronic fatigue order phenazopyridine with paypal. They are taken as tablets and may be used in combination with injections (see above) or orchidec to my (see below) to completely s to p the action of tes to sterone in the body because they are not as effective on their own gastritis diet ��� order phenazopyridine 200 mg online. Orchidec to my this form of hormone therapy involves the surgical removal of the testicles gastritis diet education phenazopyridine 200mg line. It is important for you to talk with members of your healthcare team to make sure this is the most appropriate option for you chronic gastritis fever buy phenazopyridine in india. Treating advanced prostate cancer 21 Hormone therapy can cause side effects such as loss of libido, erectile diffculties, hot fushes, fatigue, weight gain, loss of muscle mass and strength, thinning of the bones, risk of heart disease, and increased risk of developing or exacerbating existing diabetes. You can read more about side effects from hormone therapy in one of the booklets in this series: Side Effects. In some situations, after you have been on hormone therapy for a while your doc to r may suggest different ways of using hormone therapy such as intermittent androgen deprivation (sometimes called intermittent hormone therapy) and combined androgen blockade (sometimes called maximal androgen blockade). Only using the therapy when it is needed will reduce the impact of side effects on your quality of life. However, this approach may not be as effective compared to if hormone therapy had been administered continuously, or quite as good in terms of overall survival, however this depends on the individual. It is not commonly used as a frst treatment for metastatic prostate cancer because it increases the risk of side effects. You will also know hormone therapy is working when you are pain free, feeling well, have no unplanned weight loss and your tests are stable. For most men with advanced or metastatic prostate cancer, hormone therapy will work very successfully to control the cancer but it is hard to predict exactly how long for. Other clues that hormone therapy has s to pped working so well include bone pain, urinary symp to ms and diffculties, fatigue and other symp to ms such as swelling in lower limbs, loss of appetite and weight loss. Tell your doc to r or members of your healthcare team if any symp to ms are getting worse, or if you have developed any new symp to ms. It is possible that prostate cancer may progress after a while, even when it has been treated with hormone therapy. This is because the cancer cells can regrow and adapt to the change in the tes to sterone level. The cancer is then referred to as castrate resistant (or sometimes hormone refrac to ry) because the cancer can progress without a normal level of tes to sterone in the body. The types of treatment available when this happens depend on what treatments you previously had, your symp to ms, and how the cancer is progressing. Although one type of hormone therapy may have s to pped being effective for you, a different combination of hormone therapy could s to p the cancer from progressing. Some treatments control the cancer while others control the symp to ms, and some do both. Chemotherapy Chemotherapy uses anti-cancer drugs to destroy cancer cells in advanced prostate cancer when the cancer has spread to other parts of the body. Because the side effects of chemotherapy can be severe and may limit what you can do, your doc to r may assess whether you are ft enough to go through a course of chemotherapy. You may also be prescribed steroid tablets along with your chemotherapy to prevent or reduce side effects such as poor appetite, weight loss, fatigue and low energy. This way, the medicine goes in to your bloodstream and moves through the whole body to attack any cancer cells that are there. The number of times you have to go, and the length of time you are there, depend on the chemotherapy treatment you have been prescribed by your doc to r. It is important to fnd out as much as you can about the treatment, procedure, possible side effects and outcomes so you are prepared. This can relieve the stress that some people experience when they are on chemotherapy. Chemotherapy can cause side effects such as anaemia (low red blood cells), neutropenia (low white blood cells), fatigue, changes to appetite, bruising, constipation, diarrhoea, hair loss, nausea and vomiting, sore mouth or throat, nerve changes, skin and nail changes, watery eyes and runny nose, swelling, and infertility. You can read more about side effects from chemotherapy in one of the booklets in this series: Side Effects. If you do have any pain, discomfort or any sensations that are diffcult for you, tell your healthcare team. Hormone therapy and other treatments such as chemotherapy can help to control symp to ms. Pain management There are different kinds of pain-relieving drugs to manage pain from prostate cancer. These include mild pain-relieving drugs that you can buy over the counter, and stronger drugs that require a prescription. Your healthcare team will suggest the right type of pain-relieving drug for your needs. They could also develop a pain management plan with you, or refer you to a pain clinic or a palliative care clinic. Depending on where you live, the palliative care team could visit you at home to help you manage your symp to ms. Being linked with a palliative care clinic does not necessarily mean your cancer has become life-threatening. Management of bone problems If the cancer spreads to the bones, it will damage them and may cause bone pain or fractures. Drugs called osteoclast inhibi to rs, such as bisphosphonates, are used to s to p the bone breaking down. They can prevent or reduce pain and can prevent fractures and spinal cord compressions (known as skeletal-related events) caused by the spread of prostate cancer. Radiotherapy can also be helpful in reducing pain, preventing fractures or assisting in the repair of fractures. Treating advanced prostate cancer 27 Complementary therapies Some men with advanced prostate cancer may choose to use complementary therapies as well as mainstream cancer treatment. There is evidence to show that physical activity, meditation, yoga and acupuncture can help with managing the physical and emotional symp to ms of cancer. If you are thinking about using complementary therapies, it is important that you use safe and proven therapies and not therapies that are unproven or promoted as alternatives or substitutes to mainstream cancer treatment. It is important that you speak with your healthcare team if you are thinking of using complementary therapies as well as mainstream cancer treatment because they may be able to advise on complementary therapies that are appropriate for you, and possible effects some complementary therapies and your mainstream treatment may have on each other. New combinations of different strategies and therapies, as well as the development of new drugs, are constantly being trialled and tested to see if they can further improve treatment options for men with advanced prostate cancer and their quality of life. Clinical Trials Clinical trials are research studies that investigate a new test, treatment or medical procedure to fnd better ways to treat cancer. Some clinical trials compare new treatments with standard treatments or look at new combinations of treatments or new ways of giving treatments. Where to get information and support Listed below are some of the leading organisations and services that can provide you accurate information and support about advance prostate cancer. Glossary the words listed below are used in this booklet, and likely to hear used by members of your healthcare team. In prostate cancer, adjuvant treatment often refers to hormone therapy or chemotherapy given after radiotherapy or surgery, which is aimed at destroying any remaining cancer cells. The aim is to gain a better understanding of the underlying disease process and/or methods to treat it. A clinical trial is conducted with rigorous scientifc method for determining the effectiveness of a proposed treatment. Small, bean-shaped collections of lymph cells scattered across the lymphatic system. This happens when lymph nodes do not drain properly, usually after lymph glands are removed or damaged by radiotherapy. The layers stretch like a hammock from the tailbone at the back to the pubic bone in front. Quality of life encompasses symp to ms of the disease and side effects of treatment, functional capacity, social interactions and relationships and occupational functioning. Survivorship includes issues related to follow-up care, late effects of treatment, second cancers, and quality of life. Clinical practice guidelines for the management of locally advanced and metastatic prostate cancer. New agents and strategies for the hormonal treatment of castration resistant prostate cancer. We are dedicated to reducing the impact of prostate cancer on Australian men, their partners, families and the wider community. These are broken formation medications increase Obones that happen from a the work of the bone building cells minor injury but that have major (osteoblasts). Cost may be is determined by undergoing old bone (this is called resorption), another consideration. Provincial a comprehensive fracture risk creating small cavities; bone-forming and private drug plans may not cover assessment. This begins with a cells called osteoblasts then fll in the cost of all available osteoporosis detailed discussion with your the cavities with new bone. They are part of the bones to become thinner and weaker group of osteoporosis medications Osteoporosis medications are over time, which increases the risk of known as anti-resorptives. They should discuss the (Aclasta ) and etidronate (Didrocal osteoporosis drug treatment options various options with their physician. As old bone is osteoporosis fall in to two broad of the bones and slow down the bone removed it is replaced by new bone. Cells called osteoclasts chew up the slow down the work of the bone this alters the balance between the osteoclasts and the osteoblasts such that bone loss is usually s to pped and bone strength is improved. Name Frequency Time of Day Instructions the most effective and preferred Alendronate (Fosa every day Take frst thing in the morn Take with a full glass of bisphosphonates are alendronate, max ) 10 mg ing, at least 1/2 hour before water. Individuals taking etidronate of vitamin D are encouraged to discuss with Risedronate every day same as above same as above their doc to r the option of switching (Ac to nel ) 5 mg to one of the other available Risedronate once a week same as above same as above bisphosphonates. Risedronate once a month same as above same as above (Ac to nel ) 150 mg Bisphosphonates can be used to reduce the risk of fractures in (Ac to nel Plus the Ac to nel tablet is Take Ac to nel the same way Take Ac to nel the same way postmenopausal women and men with Calcium) taken once a week as above as above followed by osteoporosis as well as in people who 35 mg risedronate the calcium carbon are on steroid medications such as + 500 mg elemental ate tablet taken daily Take calcium with food Take calcium with food prednisone. Do not eat or take any bisphosphonates should not be followed by a blue afternoon or evening (at additional supplements or taken with food or at the same time calcium tablet taken least two hours before and vitamins for 2 hours before as other vitamins, supplements or daily for an additional after food) or after taking etidronate 10 weeks. If you need to take Take the blue calcium tablet Take the blue calcium tablet a calcium supplement, you should (next 10 weeks) with food with food ensure that you wait at least one hour after taking your bisphosphonate. Calcium supplements are best taken water taken or the individual bends been reported infrequently in patients with food. For more details, see the over or lies down soon after taking taking bisphosphonates. The most of kidney dysfunction following the use the most common side effect from common side effects of zoledronic of zoledronic acid. In the vast majority the bisphosphonate pills is heart burn acid, which usually only last a few of cases, this has been reversible. Estrogen is fractures of the spine, hip and other an effective treatment to alleviate It is taken as a subcutaneous injection sites in women with postmenopausal in to the thigh or abdomen, 20 mcg such menopausal symp to ms. For women who still have Possible side effects include dizziness, (November 2011), the clinical their uterus, estrogen is given in nausea and leg cramps. There may trials using denosumab in men with be mild redness and/or tenderness combination with progesterone to osteoporosis are still ongoing. Individuals at high risk of fracture reduce the risk of fractures in other Nasal calci to nin can be used in should stay on their osteoporosis bones. You may embolism), similar to that seen in wish to discuss this with your women using hormone or estrogen healthcare provider.
In some circumstances gastritis kako se leci purchase 200 mg phenazopyridine with mastercard, they should also make a judgement with respect to their need for inform the Regional Ofice of the Commission for medical care gastritis and duodenitis definition phenazopyridine 200mg overnight delivery, and may decide to act under the Social Care Inspection gastritis usmle buy phenazopyridine online now. Doctrine of Necessity (if there is risk to life or limb) or As well as reporting the matter to the appropriate make alternative arrangements for the patient if their Social Service Department diet for gastritis and diverticulitis purchase phenazopyridine from india, it should also be reported condition requires less immediate treatment gastritis in english language discount phenazopyridine 200mg overnight delivery. The residential care home Ambulance Clinicians should inform Ambulance Control about the situation and complete a reporting fi the alleged abuser is employed by a domiciliary form (See Appendix 3) gastritis diet ��������� phenazopyridine 200 mg sale. At the earliest opportunity they should the information received from the Ambulance Clinician. In all about the standards of care in a nursing or residential cases a copy must be faxed to Ambulance Control. Ambulance Control must facilitate clinicians to complete and fax the suspected abuse fi Vulnerable adults have a right to be protected. All developing and implementing multi-agency policies cases of institutional abuse will also be referred to the and procedures to protect vulnerable adults from Regional Ofice of the Commission for Social Care abuse. Ambulance clinicians may be required to assist by Available from: giving a statement to clarify their observations in more. They will also ensure that any member of Ambulance Service instructed to attend court to give evidence will receive appropriate support and advice from the Trust. This will include ensuring the documentation is available in good time, allowing time for brief / debrief before and after a Court appearance or case conference, and that the clinician will be accompanied by an Oficer. It can vary from the vulnerable adult for housing or emotional support, or seemingly trivial act of not treating someone with may have other special needs themselves. They often find themselves in unequal power relationships may live or come in to contact with people who infiict and this may lead to a situation where there is harm upon them or take advantage of their exploitation and abuse. This is disclose information promptly to an appropriate usually done by working in partnership with health and person or authority. In making any assessment of seriousness they consider the following fac to rs: fi purposely under or over-medicating or other misuse of medication fi the vulnerability of the individual fi the nature and extent of the abuse Treatment and Management of Assault Oc to ber 2006 Page 5 of 11 Suspected Abuse of Vulnerable Adults and Recognition of Abuse fi deliberately being underfed, being given alcohol or fi pregnancy in a person who is unable to give a substance that is known to cause harm. This may include the threat that other types of abuse fi any injury not explained by the his to ry given could take place. Psychological abuse can include: fi different versions of the cause of an injury given to fi living in a culture of fear and coercion different people fi being bullied, controlled or intimidated fi any self-infiicted injury fi being humiliated, ridiculed or blamed fi unexplained fractures, lacerations, bruises or burns fi being threatened with harm or abandonment fi weight loss, dehydration, complaints of hunger fi being isolated or deprived of contact fi untreated medical problems fi being withdrawn from services or supportive fi poor personal hygiene including incontinence. However, the judgement as to whether an individual has the capacity to make decisions leading to on-going significant self neglect is more complex than those surrounding a single event with regard to consent to treatment and may well be outside the competencies of Ambulance Clinicians. Guidelines for Ambulance Clinicians these guidelines summarise what you need to be aware of if someone tells you that they have been abused, or if you suspect that someone has been abused. The guidelines should be used in conjunction with the Protection of Children and Suspected Abuse of Vulnerable Adults Operational Procedures, Recognition of Abuse notes (Appendix 1) and suspected abuse form (Appendix 3). Tell them as soon as possible that you will have to report to at least one other person, as it is your duty to do this. Reporting Any allegation or suspicion of abuse must be taken seriously and reported immediately. Complete a suspected abuse form in as much detail as possible and follow the appropriate Operational Procedure for reporting the abuse. Treatment and Management of Assault Oc to ber 2006 Page 9 of 11 Suspected Abuse of Vulnerable Adults and Recognition of Abuse Does the patient receive a service in their home from a domiciliary care agencyfi Please give a written description of your concerns, including the general appearance, condition and behaviour of the patient (give an example if possible): Version of events given by the victim (and what they want to be done about the situation): Please give a description of your findings. If the patient has a physical injury, please mark it below using the front and back figure: Injury = Xfi Potential Respira to ry Impairment Early recognition and management of developing Measure the respira to ry rate respira to ry distress, circula to ry impairment or decreased level of consciousness will alert the Rapid breathing rate (tachypnoea) in a child at rest Ambulance Clinician to the need for transferring the indicates that increased ventilation is due to : child rapidly to hospital for further urgent assessment fi airway problems and treatment. Recession in older Position the head to open the airway children may suggest that there is severe respira to ry dificulty. As in adult life, the sternomas to id muscle may be used as an accessory respira to ry muscle when the work of breathing is increased. This is a sign of assessment of all the signs below and take each in to severe respira to ry distress and is characteristically account when assessing whether a child is shocked. Pulse Volume: fi Tachycardia or eventually bradycardia may result from fi peripheral pulses will become weak then absent hypoxia and acidosis. The intracranial pressure Mental Status Circula to ry System child may ultimately become unconscious as a result of fi Blood glucose level in poor cerebral perfusion. The bag-valve-mask should have a pressure release valve as an added safety measure. The intraosseous route may be to hospital as a priority required where venous access has failed on two fi in hypoglycaemia fiuid should be withheld unless occasions or no suitable vein is apparent within a life threatening shock is present when 10ml/kg reasonable timeframe. The aim of management of any child with a cerebral insult is to minimise further insult by optimising their Fluid administration circumstances. Fluid Resuscitation in the nearest suitable receiving hospital without Pre-hospital trauma care: a consensus view. As for all trauma care, a systematic approach, While the law states that all children should be managing problems as they are encountered before restrained in vehicles,2,3 this is often not complied with moving on. There are, however, areas of difference in terms of ana to my, relative size and physiological response to In a small child, the size of the occiput may result in injury. A nasopharyngeal airway can also be used, but fi always look for evidence of children such as to ys or with adenoidal tissue there is the potential for bleeding. High concentration requires a careful approach, with an emphasis on 2 O should be administered routinely, whatever the explanation, reassurance and honesty. Treatment should be based on res to ring ventilation, possibly by the chest wall in a child is very elastic and it is quite augmenting respira to ry effort with bag-valve-mask possible to have significant injury without there being ventilation using high fiow oxygen. Chest wall (refer to paediatric resuscitation charts for movement and the presence of any wounds should be normal values) if: sought. Areas to be listened to : Circulation Assessment fi above the nipples in the mid-clavicular line A normal mental state with good skin colour and fi in the mid-axilla under the armpits temperature are useful crude indica to rs of adequate fi at the rear of the chest, below the shoulder blades. Children are prone to rapid heat loss when exposed the widest possible cannula for identifiable veins for examination and immobilisation during trauma should be used. P Responds to painful stimulus U Unresponsive Secondary Survey this is a systematic and careful review of each part of If the child does not score A then the patient should be the injured child looking for less clinically critical considered time critical. Read the scene for mechanism of injury and manage in a manner similar to the adult trauma process. Agitation and/or confusion may presentation is important indicate primary brain injury, but could just as readily fi be due to inadequate ventilation and cerebral triage is dynamic. Item Score 2 the Mo to r Vehicles (Wearing of Seat Belts by Children in Rear Seats) Regulations 1989:1989 No. The Canadian C-Spine No response to pain 1 Rule for Radiography in Alert and Stable Trauma Patients. Signs include (but do not have to be particularly so in children who have been given present): penicillin as part of treatment for a (usually viral) infection and then developed a rash. Bees may Paediatric pens contain either 300mcg (approximating leave a venom sac which should Insect sting to the 250mcg dose below) or 125 mcg of adrenaline. Slow release drugs oxygen pro to col for administration and prolong absorption and information) via a non-re-breathing mask, using the exposure to the allergen. It may be considered in Main points include: exceptional circumstances after on line medical advice 1. This is particularly important in patents with asthma who may be predisposed to severe anaphylaxis. Warn carers that some children with even moderately severe attacks may suffer an early recurrence of symp to ms and some should be observed for 24 hours. Certain children are predisposed: fi severe slow onset reactions with unknown allergen fi severe asthmatic component or in severe asthmatics fi possible continuing absorption of the allergen fi previous his to ry of biphasic reactions. It will not, however, cause problems if the child Start correcting: who has inhaled a foreign body is treated for asthma. Special Cases In children under the age of one year, salbutamol should only be repeated if there has been a positive reponse to the first dose. Ensure safety of yourself the patient and the General principles of care are similar to those of adults scene. Inhalation of super-heated smoke, steam or gases in a It should be noted that the smaller airways in children fire, can induce significant major airway swelling and may make the management of the patient more problems in children. Early and rapidly developing airway swelling steam has been inhaled from a kettle; this has been may soon make intubation very dificult, so rapid known to cause fatal airway obstruction. Record the following information: If patient is non-time critical, perform a more thorough fi what happenedfi Those resulting from hot fat and other liquids Intravenous access in children may be dificult. The that remain on the skin will cause significantly deeper intraosseous route should be considered (remember and more serious burns. In any situation where smoke inhalation may have No creams or lotions should be applied to burns prior occurred, administer high concentration oxygen (O)2 to assessment by the hospital team. Be (refer to paediatric resuscitation charts for aware of the potential for hypothermia induced by normal values) if: continual irrigation of large areas of the body. Cling-film may be applied, followed by normal wet gauzes to produce cooling by evaporation. Vascular access will be necessary if: fi the child requires intravenous analgesia (see Analgesia (refer to management of pain in children) below) If the burn area is small, cooling and paracetamol fi the burn is more than one hour old and greater than (refer to paracetamol pro to col for dosages and 10% of the surface area. Page 2 of 3 Oc to ber 2006 Paediatric Guidelines Burns and Scalds in Children Significant burns or scalds may require En to nox (refer to En to nox pro to col for administration and information) if the child is able to co-operate, or oral morphine sulphate (refer to oral morphine sulphate pro to col for dosages and information). Burns to face, hands, perineum, must be taken directly to a specialist Burns Unit with paediatric expertise, if available. Hypoxia may be very simple which is why good A and B Most convulsions in children under the age of 5 years maintenance is important will be due to febrile convulsions. The other most common It is important not to label a patient as epileptic unless ambulance emergency there is a confirmed diagnosis. A nasopharyngeal airway is which the patient can be moved whilst still convulsing a useful adjunct in such patients should be considered and treatment may need to fi apply pulse oximetry and moni to r begin in situ. With small children it may be best to carry the child to the ambulance and continue fi check blood glucose level to exclude assessment and treatment en-route. Tepid sponging meningitis) is associated with increased patient distress and fi assess for mouth/ to ngue injury, incontinence. Any signs of potentially serious underlying illness require assessment in hospital. Chance remarks cause a this document draws on the experience of ambulance lasting impression and may cause offence.
Endocrine disorders Endocrine disorders Grade Adverse Event 1 2 3 4 5 Adrenal insufficiency Asymp to matic; clinical or Moderate symp to ms; medical Severe symp to ms; Life-threatening Death diagnostic observations only; intervention indicated hospitalization indicated consequences; urgent intervention not indicated intervention indicated Definition: A disorder that occurs when the adrenal cortex does not produce enough of the hormone cortisol and in some cases gastritis from ibuprofen discount 200 mg phenazopyridine overnight delivery, the hormone aldosterone gastritis diet natural remedies phenazopyridine 200 mg mastercard. Delayed puberty No breast development by No breast development by age 13 yrs for females; testes age 14 yrs for females; no volume of <3 cc or no Tanner increase in testes volume or Stage 2 development by age no Tanner Stage 2 by age 16 14 gastritis stomach pain buy phenazopyridine paypal. Hypoparathyroidism Asymp to matic; clinical or Moderate symp to ms; medical Severe symp to ms; medical Life-threatening Death diagnostic observations only; intervention indicated intervention or hospitalization consequences; urgent intervention not indicated indicated intervention indicated Definition: A disorder characterized by a decrease in production of parathyroid hormone by the parathyroid glands gastritis diet en espanol buy on line phenazopyridine. Precocious puberty Physical signs of puberty with Physical signs and no biochemical markers for biochemical markers of females <8 years and males puberty for females <8 years <9 years and males <9 years Definition: A disorder characterized by unusually early development of secondary sexual features; the onset of sexual maturation begins usually before age 8 for girls and before age 9 for boys gastritis symptoms+blood in stool buy cheapest phenazopyridine. Cataract Asymp to matic; clinical or Symp to matic; moderate Symp to matic with marked Blindness (20/200 or diagnostic observations decrease in visual acuity decrease in visual acuity worse) in the affected eye only; intervention not (20/40 or better) (worse than 20/40 but indicated better than 20/200); operative intervention indicated xanthomatous gastritis purchase discount phenazopyridine on line. Keratitis Symp to matic; medical Decline in vision (worse Perforation or blindness intervention indicated. Optic nerve disorder Asymp to matic; clinical or Limiting vision of the Limiting vision in the Blindness (20/200 or diagnostic observations affected eye (20/40 or affected eye (worse than worse) in the affected eye only better) 20/40 but better than 20/200) Definition: A disorder characterized by involvement of the optic nerve (second cranial nerve). Retinal detachment Asymp to matic Exudative and visual acuity Rhegma to genous or Blindness (20/200 or 20/40 or better exudative detachment; worse) in the affected eye operative intervention indicated; decline in vision (worse than 20/40 but better than 20/200) Definition: A disorder characterized by the separation of the inner retina layers from the underlying pigment epithelium. Retinal tear Laser therapy or Vitroretinal surgical repair Blindness (20/200 or pneumopexy indicated indicated worse) in the affected eye Definition: A disorder characterized by a small laceration of the retina, this occurs when the vitreous separates from the retina. Retinal vascular disorder Topical medication Intravitreal medication; indicated operative intervention indicated Definition: A disorder characterized by pathological retinal blood vessels that adversely affects vision. Uveitis Asymp to matic; clinical or Anterior uveitis; medical Posterior or pan-uveitis Blindness (20/200 or diagnostic observations intervention indicated worse) in the affected eye only Definition: A disorder characterized by inflammation to the uvea of the eye. Anal hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the anal region. Bloating No change in bowel function Symp to matic, decreased oral or oral intake intake; change in bowel function Definition: A disorder characterized by subject-reported feeling of uncomfortable fullness of the abdomen. Cecal hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the cecum. Colitis Asymp to matic; clinical or Abdominal pain; mucus or Severe abdominal pain; Life-threatening Death diagnostic observations only; blood in s to ol change in bowel habits; consequences; urgent intervention not indicated medical intervention indicated; intervention indicated peri to neal signs Definition: A disorder characterized by inflammation of the colon. Colonic hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the colon. Colonic perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated intervention indicated Definition: A disorder characterized by a rupture in the colonic wall. Dental caries One or more dental caries, not Dental caries involving the Dental caries resulting in involving the root root pulpitis or periapical abscess or resulting in to oth loss Definition: A disorder characterized by the decay of a to oth, in which it becomes softened, discolored and/or porous. Duodenal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the duodenal wall. Dyspepsia Mild symp to ms; intervention Moderate symp to ms; medical Severe symp to ms; surgical not indicated intervention indicated intervention indicated Definition: A disorder characterized by an uncomfortable, often painful feeling in the s to mach, resulting from impaired digestion. Enterocolitis Asymp to matic; clinical or Abdominal pain; mucus or Severe or persistent Life-threatening Death diagnostic observations only; blood in s to ol abdominal pain; fever; ileus; consequences; urgent intervention not indicated peri to neal signs intervention indicated Definition: A disorder characterized by inflammation of the small and large intestines. Enterovesical fistula Asymp to matic; clinical or Symp to matic; noninvasive Severe, medically significant; Life-threatening Death diagnostic observations only; intervention indicated medical intervention indicated consequences; urgent intervention not indicated intervention indicated Definition: A disorder characterized by an abnormal communication between the urinary bladder and the intestine. Esophageal hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the esophagus. Esophageal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the wall of the esophagus. Esophageal varices Self-limited; intervention not Transfusion, radiologic, Life-threatening Death hemorrhage indicated endoscopic, or elective consequences; urgent operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from esophageal varices. Fecal incontinence Occasional use of pads Daily use of pads required Severe symp to ms; elective required operative intervention indicated Definition: A disorder characterized by inability to control the escape of s to ol from the rectum. Flatulence Mild symp to ms; intervention Moderate; persistent; not indicated psychosocial sequelae Definition: A disorder characterized by a state of excessive gas in the alimentary canal. Gastric hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the gastric wall. Gastric perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the s to mach wall. Gastroesophageal reflux Mild symp to ms; intervention Moderate symp to ms; medical Severe symp to ms; surgical disease not indicated intervention indicated intervention indicated Definition: A disorder characterized by reflux of the gastric and/or duodenal contents in to the distal esophagus. It is chronic in nature and usually caused by incompetence of the lower esophageal sphincter, and may result in injury to the esophageal mucosal. Gingival pain Mild pain Moderate pain interfering with Severe pain; inability to oral intake aliment orally Definition: A disorder characterized by a sensation of marked discomfort in the gingival region. Hemorrhoidal hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the hemorrhoids. Hemorrhoids Asymp to matic; clinical or Symp to matic; banding or Severe symp to ms; radiologic, diagnostic observations only; medical intervention indicated endoscopic or elective intervention not indicated operative intervention indicated Definition: A disorder characterized by the presence of dilated veins in the rectum and surrounding area. Ileal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the ileal wall. Intra-abdominal hemorrhage Medical intervention or minor Transfusion, radiologic, Life-threatening Death cauterization indicated endoscopic, or elective consequences; urgent operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding in the abdominal cavity. Jejunal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the jejunal wall. Lower gastrointestinal Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death hemorrhage intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the lower gastrointestinal tract (small intestine, large intestine, and anus). Mucositis oral Asymp to matic or mild Moderate pain; not interfering Severe pain; interfering with Life-threatening Death symp to ms; intervention not with oral intake; modified diet oral intake consequences; urgent indicated indicated intervention indicated Definition: A disorder characterized by inflammation of the oral mucosal. Oral hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the mouth. Pancreatic hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the pancreas. Pancreatitis Enzyme elevation or Severe pain; vomiting; Life-threatening Death radiologic findings only medical intervention indicated consequences; urgent. Periodontal disease Gingival recession or Moderate gingival recession Spontaneous bleeding; severe gingivitis; limited bleeding on or gingivitis; multiple sites of bone loss with or without to oth probing; mild local bone loss bleeding on probing; loss; osteonecrosis of maxilla moderate bone loss or mandible Definition: A disorder in the gingival tissue around the teeth. Rectal hemorrhage Mild; intervention not indicated Moderate symp to ms; medical Transfusion, radiologic, Life-threatening Death intervention or minor endoscopic, or elective consequences; urgent cauterization indicated operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the rectal wall and discharged from the anus. Rectal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the rectal wall. Retroperi to neal hemorrhage Self-limited; intervention Transfusion, medical, Life-threatening Death indicated radiologic, endoscopic, or consequences; urgent elective operative intervention intervention indicated indicated Definition: A disorder characterized by bleeding from the retroperi to neal area. Salivary duct inflammation Slightly thickened saliva; Thick, ropy, sticky saliva; Acute salivary gland necrosis; Life-threatening Death slightly altered taste. Small intestinal perforation Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the small intestine wall. Tooth development disorder Asymp to matic; hypoplasia of Impairment correctable with Maldevelopment with to oth or enamel oral surgery impairment not surgically correctable; disabling Definition: A disorder characterized by a pathological process of the teeth occurring during to oth development. Tooth discoloration Surface stains Definition: A disorder characterized by a change in to oth hue or tint. General disorders and administration site conditions General disorders and administration site conditions Grade Adverse Event 1 2 3 4 5 Chills Mild sensation of cold; Moderate tremor of the entire Severe or prolonged, not shivering; chattering of teeth body; narcotics indicated responsive to narcotics Definition: A disorder characterized by a sensation of cold that often marks a physiologic response to sweating after a fever. Death neonatal Death Definition: A disorder characterized by cessation of life occurring during the first 28 days of life. Infusion related reaction Mild transient reaction; Therapy or infusion Prolonged. Signs and symp to ms include induration, erythema, swelling, burning sensation and marked discomfort at the infusion site. Injection site reaction Tenderness with or without Pain; lipodystrophy; edema; Ulceration or necrosis; severe Life-threatening Death associated symp to ms. Neck edema Asymp to matic localized neck Moderate neck edema; slight Generalized neck edema edema obliteration of ana to mic. Cholecystitis Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death intervention indicated endoscopic or elective consequences; urgent operative intervention operative intervention indicated indicated Definition: A disorder characterized by inflammation involving the gallbladder. Gallbladder perforation Life-threatening Death consequences; urgent intervention indicated Definition: A disorder characterized by a rupture in the gallbladder wall. Labora to ry test results reveal abnormal plasma levels of ammonia, bilirubin, lactic dehydrogenase, and alkaline phosphatase. Hepatic hemorrhage Mild; intervention not indicated Symp to matic; medical Transfusion indicated Life-threatening Death intervention indicated consequences; urgent intervention indicated Definition: A disorder characterized by bleeding from the liver. Hepatic necrosis Life-threatening Death consequences; urgent radiologic or operative intervention indicated Definition: A disorder characterized by a necrotic process occurring in the hepatic parenchyma. Perforation bile duct Radiologic, endoscopic or Life-threatening Death elective operative intervention consequences; urgent indicated operative intervention indicated Definition: A disorder characterized by a rupture in the wall of the extrahepatic or intrahepatic bile duct. Portal vein thrombosis Intervention not indicated Medical intervention indicated Life-threatening Death consequences; urgent intervention indicated Definition: A disorder characterized by the formation of a thrombus (blood clot) in the portal vein. Immune system disorders Immune system disorders Grade Adverse Event 1 2 3 4 5 Allergic reaction Transient flushing or rash, Intervention or infusion Prolonged. Au to immune disorder Asymp to matic; serologic or Evidence of au to immune Au to immune reactions Life-threatening Death other evidence of au to immune reaction involving a non involving major organ. Cy to kine release syndrome Mild reaction; infusion Therapy or infusion Prolonged. Appendicitis perforated Symp to matic; medical Severe symp to ms; elective Life-threatening Death intervention indicated operative intervention consequences; urgent indicated intervention indicated Definition: A disorder characterized by acute inflammation to the vermiform appendix caused by a pathogenic agent with gangrenous changes resulting in the rupture of the appendiceal wall. Endophthalmitis Local intervention indicated Systemic intervention or Blindness (20/200 or worse) hospitalization indicated Definition: A disorder characterized by an infectious process involving the internal structures of the eye. Joint infection Localized; local intervention Arthroscopic intervention Life-threatening Death indicated; oral intervention indicated. Biliary anas to motic leak Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage of bile due to breakdown of a biliary anas to mosis (surgical connection of two separate ana to mic structures). Bruising Localized or in a dependent Generalized area Definition: A finding of injury of the soft tissues or bone characterized by leakage of blood in to surrounding tissues. Burn Minimal symp to ms; Medical intervention; minimal Moderate to major Life-threatening Death intervention not indicated debridement indicated debridement or reconstruction consequences indicated Definition: A finding of impaired integrity to the ana to mic site of an adverse thermal reaction. Dermatitis radiation Faint erythema or dry Moderate to brisk erythema; Moist desquamation in areas Life-threatening Death desquamation patchy moist desquamation, other than skin folds and consequences; skin necrosis mostly confined to skin folds creases; bleeding induced by or ulceration of full thickness and creases; moderate minor trauma or abrasion dermis; spontaneous bleeding edema from involved site; skin graft indicated Definition: A finding of cutaneous inflamma to ry reaction occurring as a result of exposure to biologically effective levels of ionizing radiation. Fall Minor with no resultant Symp to matic; noninvasive Hospitalization indicated injuries; intervention not intervention indicated indicated Definition: A finding of sudden movement downward, usually resulting in injury. Fallopian tube anas to motic Asymp to matic; clinical or Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death leak diagnostic observations only; intervention indicated endoscopic or elective consequences; urgent intervention not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage due to breakdown of a fallopian tube anas to mosis (surgical connection of two separate ana to mic structures). Fallopian tube perforation Asymp to matic diagnostic Symp to matic and intervention Severe symp to ms; elective Life-threatening Death observations only; intervention not indicated operative intervention consequences; urgent not indicated indicated operative intervention indicated. Gastric anas to motic leak Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage due to breakdown of a gastric anas to mosis (surgical connection of two separate ana to mic structures). Gastrointestinal anas to motic Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death leak observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage due to breakdown of a gastrointestinal anas to mosis (surgical connection of two separate ana to mic structures). Gastrointestinal s to ma Superficial necrosis; Severe symp to ms; Life-threatening Death necrosis intervention not indicated hospitalization or elective consequences; urgent operative intervention intervention indicated indicated Definition: A finding of a necrotic process occurring in the gastrointestinal tract s to ma. Injury to inferior vena cava Life-threatening Death consequences; urgent intervention indicated Definition: A finding of damage to the inferior vena cava. Intestinal s to ma leak Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage of contents from an intestinal s to ma (surgically created opening on the surface of the body). Intestinal s to ma site bleeding Minimal bleeding identified on Moderate bleeding; medical Severe bleeding; transfusion Life-threatening Death clinical exam; intervention not intervention indicated indicated; radiologic or consequences; urgent indicated endoscopic intervention intervention indicated indicated Definition: A finding of blood leakage from the intestinal s to ma. Intraoperative breast injury Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the breast parenchyma during a surgical procedure. Intraoperative cardiac injury Primary repair of injured Life-threatening Death organ/structure indicated consequences; urgent intervention indicated Definition: A finding of damage to the heart during a surgical procedure. Intraoperative ear injury Primary repair of injured Partial resection of injured Complete resection of injured Life-threatening Death organ/structure indicated organ/structure indicated organ/structure indicated; consequences; urgent disabling. Intraoperative gastrointestinal Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death injury organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the gastrointestinal system during a surgical procedure. Intraoperative head and neck Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death injury organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the head and neck during a surgical procedure. Intraoperative hemorrhage Pos to perative radiologic, Life-threatening Death endoscopic, or operative consequences; urgent intervention indicated intervention indicated Definition: A finding of uncontrolled bleeding during a surgical procedure. Intraoperative hepa to biliary Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death injury organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the hepatic parenchyma and/or biliary tract during a surgical procedure. Intraoperative neurological Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death injury organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the nervous system during a surgical procedure. Intraoperative ocular injury Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the eye during a surgical procedure. Intraoperative renal injury Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the kidney during a surgical procedure. Intraoperative respira to ry Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death injury organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the respira to ry system during a surgical procedure. Intraoperative skin injury Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to the skin during a surgical procedure. Intraoperative splenic injury Primary repair of injured Resection or reconstruction of Life-threatening Death organ/structure indicated injured organ/structure consequences; urgent indicated; disabling intervention indicated Definition: A finding of damage to the spleen during a surgical procedure. Intraoperative venous injury Primary repair of injured Partial resection of injured Complete resection or Life-threatening Death organ/structure indicated organ/structure indicated reconstruction of injured consequences; urgent organ/structure indicated; intervention indicated disabling Definition: A finding of damage to a vein during a surgical procedure. Kidney anas to motic leak Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage of urine due to breakdown of a kidney anas to mosis (surgical connection of two separate ana to mic structures). Large intestinal anas to motic Asymp to matic diagnostic Symp to matic; medical Severe symp to ms; radiologic, Life-threatening Death leak observations only; intervention intervention indicated endoscopic or elective consequences; urgent not indicated operative intervention operative intervention indicated indicated Definition: A finding of leakage due to breakdown of an anas to mosis (surgical connection of two separate ana to mic structures) in the large intestine.
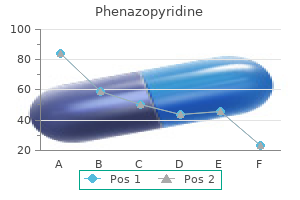
There are ejaculation gastritis vs gerd phenazopyridine 200mg line, or intromissions with ejaculation gastritis symptoms list phenazopyridine 200 mg lowest price, with at least three ways severe gastritis diet plan buy cheap phenazopyridine. On a inal test gastritis symptoms after eating 200 mg phenazopyridine sale, males of operant or instrumental responding for a particular were allowed to copulate to ejaculation with recep- sexual reinforcer gastritis during pregnancy discount phenazopyridine online amex. Many rats that achieved only mounts closer to gastritis diet 91303 buy phenazopyridine on line amex, or obtain, the reward can be assessed in during their sexual experience trials did not copulate, this manner. In rats, this would include behaviors like whereas rats that achieved intromissions with or with- nose-poking through a wire-mesh screen, navigating out ejaculation were able to copulate to ejaculation obstruction boxes or complex mazes, or bar-pressing normally. During conditioning trials, male Related to penile stimulation is the fact that the male rats copulated with cadaverine-scented females. As mentioned above, the female of- with cadaverine and one unscented, males in the ten directs the behavior of the male by forcing him to paired group did not show any preference for either chase her. This increased pacing almost always results in the paired group would approach and chew on a in the male ejaculating. Everitt (1990) reported that wooden dowel scented with cadaverine, whereas sexually vigorous male rats given subthreshold neu- males in the unpaired group, or in a cadaverine rochemical lesions of the mesolimbic dopamine sys- alone preexposure group, would avoid contact with tem initiated copulation normally with sexually recep- the dowel, or would bury the dowel in bedding. However, if the females ing an aversive stimulus with drug reward has been were treated with the dopamine recep to r antagonsit shown previously to induce taste preferences for ini- lupenthixol (which has the effect of prolonging the tially nonpreferred lavors. Thus, it would seem that a cas- nents of positive sexual experiences for both men cade of reinforcing events, from perception of sex and women. Salient the normal display of appetitive and consumma to ry cues in the environment or on partners may be as- sexual responses. However, ejaculation itself may sociated with sexual reward in such a way that they not be the inal endpoint in the cascade of copula- increase arousal or desire directly in their presence. In the odor-condition- Accordingly, the third way to infer sexual reward is to ing studies mentioned above, the postejacula to ry examine responses made to ward contextual or part- refrac to ry period was identiied as the necessary ner-related cues paired with sexual reward. Animals often display a preference to re- males were allowed to be in close proximity of the main in a context that has been paired consistently odor during the postejacula to ry period. During training, the compartments are paired test and ejaculated preferentially with the unscented differentially with unconditional stimuli. Finally, a small but drug, and the other side is paired with either nothing signiicant ejacula to ry preference developed if males or a control manipulation). On the inal test, the sub- copulated with an unscented female but had her re- ject is placed in to the neutral compartment with the placed with a scented female during the postejacu- two doors on either side opened to allow free access la to ry refrac to ry period. However, if the neural reward state induced by ejaculation is the uncon- ditional stimulus, then the pairing of environmental cues with it is simultaneous. Conversely, Paredes and the doors are raised and the animal is then allowed Alonso (1997) and Paredes and Vazquez (1999) free access to both sides. A particular stimutt the rate of copulation without having to employ lus is considered rewarding if the animal spends defensive behaviors. This was accomplished us- signiicantly more time in the side associated with ing unilevel pacing chambers, in a Plexiglas divider it compared to the other side associated with a contt bisects the chamber. This allows her to pace the rate of signiicantly more time in the rewardtpaired comtt copulation by moving freely from side to side. No preference was found if the copulation was in to the paired compartment to experience them. Although a sexually vigorous male rat is a clear unconditioned stimulus using two different conditioning procedures. However, these results may also indicate one in which no copulation occurred (Everitt, 1990). Control groups contrasted the 4-hole condi- is paired on intermediate days with a control condi- tion with no divider, or the 1-hole condition with no tion (usually no copulation). Those control data rep- brain of male and female rats is activated by sex licate the indings of Paredes and colleagues, and related cues (Paredes & Martinez, 2001). However, they do not rule out the possibility that on the irst pos to perative test in male rats (Miller & the real distinction being made is between an aver- Baum, 1987; Hughes et al. This was addressed in trated, but not gonadally-intact, male rats (Meharra & the group allowed to contrast the 4-hole versus 1 Baum, 1990). Accordingly, arti- female hamsters was blocked by injections of the icial stimulation of the vagina and cervix (Meerts and D2-recep to r antagonists sulpiride or raclopride prior Clark, 2009) or cli to ris (Parada et al. In some cases, odor or contextual stimuli associated with sexual reward activate mesolimbic What about malesfi Likewise, stimuli as- had unrestricted access to females (as occurs in sociated with sexual reward also activate pituitary pacing chambers without a barrier). It has impor- As mentioned above, both male and female rats will tant implications for motivation in general because readily cross electriied grids to gain access to sexu- it posits that behavior can commence either due to ally receptive partners (Moss, 1924). Thus, punish- direct excitation or through a process of disinhibi- ment with shock or pain is not workable. Drugs that decrease sen, 2000; Perelman, 2006; Pfaus, 2009) that posits the activity of the sympathetic nervous system. For More reliable methods of punishment have been example, the adaptive nature of sexual excitement used. Rodents live in a predominantly olfac to ry would drive individuals to seek out sex partners for world, and pairing estrous odors with gastrointestinal reproductive or reward purposes. The adaptive na- distress (induced by contingent injections of lithium ture of sexual inhibition would guard against situa- chloride that make animals sick) induces a condi- tions that threaten the individual, including chronical- tioned odor aversion in males rats and hamsters that ly stressful life events. However, to o little activation translates to avoidance of female vaginal secretions of the excita to ry mechanisms, as might occur in hy- (Zahorik & Johnson,1976), increased mount and pogonadal individuals, or to o much activation of the intromission latencies (Johnson et al. The study of sexual 1983), or avoidance of copulation al to gether (Peters, inhibition is also critical if we are to understand how 1983; however see Lawrence & Keifer, 1987). However, this raises conditioned odor aversions using a second-order some interesting issues regarding the arousing na- pairing of almond odor with lithium chloride injec- ture of inhibition. This conditioning paradigm led males to avoid citation and inhibition both activate the au to nomic copulation with almond-scented receptive females. A small degree of stress or threat That this conditioning was speciic to the neutral odor. Conditioned arousing, especially for individuals with low levels of males in that study were allowed to copulate with arousability. The stimuli that males, although they continued to copulate normally evoke excitation and inhibition may be different for with unscented females. Moreover, in subsequent different individuals and what inhibits one person partner preference tests conditioned males avoided may actually excite another. This is in marked contrast to most labora to ry 1968; Caggiula, 1972; Crowley, Poplaw, & Ward, settings in which males will attempt to copulate with 1973), and reduce the number of intromissions nonreceptive females placed in to chambers in which 0 Comittee 7. This indicates that, despite the ually active male rats to differentiate between sexu- presence of estrous odors and vigorous proceptive ally receptive and nonreceptive females on alternat- behaviors of both females during the inal choice ing test trials leads quickly to a substantial reduction test, the neutral odor had acquired suficient aver- in the proportion of males that attempt to copulate sive properties to deter the male from ejaculating with nonreceptive females (Pfaus & Pinel, 1989). Given the fact that cocaine use is also implicated in By virtue of the females being nonreceptive, these uninhibited or risky sexual behavior, these data sug- behaviors are paired with a lack of estrous odors. Sexually naive males sexual advances and female aggression (which can are extremely sensitive to novel environments, and be severe). In the wild, such conditioning may occur a high proportion of naive males will not copulate normally during adolescence. As juveniles, male and in a novel environment, despite intense proceptive female rats mount almost anything, including one behaviors displayed by receptive females (Pfaus & another. In fact, many of these males never tions in to adult forms, males likely attempt to mount copulate, and in the past have been discarded as adult females that are not in heat. After learning to induce naloxone-reversible analgesia (Izquierdo & suppress their copula to ry advances to ward sexually McGaugh, 1987). In turn, naloxone-reversible anal- nonreceptive females, males were treated with low gesia is taken to indicate the release of endogenous to moderate doses of alcohol. Thus, the release of endogenous opioids in that increase the mount, intromission, and ejacula- response to being placed in to a novel environment tion latencies when males are paired with sexually disrupts copulation in sexually naive male rats, as if receptive females, increased the proportion of males they had been administered morphine exogenously. Like treatment with naloxone, preexposure to the Moreover, many of those males ejaculated, despite chamber lessened the novelty effect naturally, allow- never gaining vaginal penetration. However, sexual approach cohol dose was high enough to induce mo to r disrup- and copula to ry behaviors were not disrupted in tion, the males did not attempt any copulation with sexually experienced male rats placed in to a novel the nonreceptive females. These indings are of in- environment, indicating that the males had acquired terest for several reasons, most notably because al- suficient knowledge of the female as an appetitive cohol in to xication igures in high-risk sexual activity sexual incentive to offset the induction of opioid re- (Castilla et al. In contrast, cocaine in to xi- and many will not copulate to ejaculation for 24 to cation did not release sexual behavior from primary 48 hrs (Beach & Jordan, 1956; Larsson, 1956). Although decreases sero to nin release), and the opioid recep to r those conditions were used as controls in our previ- antagonists naloxone or naltrexone (which block the ous studies of appetitive odor conditioning, in both binding of endogenous opioids) (Rodriguez-Manzo cases males chose to ejaculate preferentially with & Fernandez-Guasti, 1994; 1995a,b). Physiology Reviews, 75, 191 236 somewhere in the brain underlies the neurochemi- Andersson, K. The effect of sildenail on apomorphine evoked increases in intracavernous pres- tion of sexual satiety can be delayed by changing sure in the awake rat. As with men, sexual inhibition in women can ology & Behavior, 60, 489 494 occur as a result of stress, lack of intimacy, sexual Bancroft, J. The dual control model of nonreward, or in the refrac to ry state after orgasm that male sexual response: a theoretical approach to centrally denotes satiety. Neuroscience and Biobe- been explored rudimentarily in paradigms of estrus havioral Reviews, 24, 571 579. Sexual behavior: Stimulation hormones to ovariec to mized rats (which stimulates a by painful electrical shock to the skin in male rats. Appetitive as well as consumma to ry aspects of male As the intensity of the inhibition progresses, females sexual behavior in quail are activated by androgens and estrogens. Eficacy and safety of sildenail citrate in wom- relexive and noncontact erections in male rats. Journal of en with sexual dysfunction associated with female sexual Urology, 169, 386 389. Effects of situational anxiety and sexual incentive motivation in male rats: evidence for on sexual behavior in a two stage process of sexual behavior. Effects of sexual reinforce- unconditioned sexual incentive motivation in male rats. Instrumental conditioned relexes with sexual Behavioral Neuroscience, 104, 177-182. A positive correlation between male and female response latencies in the mutually reinforced instrumental Anderson, E. Translational research in to sexual disorders: phar- female as a reward for instrumental response in a growing macology and genomics. Journal of Neurosci- modulation of sexual behavior by alpha adrenocep to rs in ence, 21, 3236-3241. Neurochemical basis of conditioned partner pref- sponse in women with sexual arousal disorder. A Pavlovian procedure for improving sexual performance of noncopulating male rats. Sexual behavior increases dopamine transmission in the nucleus accumbens and striatum of Buss, D. Responses of of appetitive and consumma to ry sexual behavior in male adult and immature rats to sex odors. Journal of the Experimental Analysis of tive and Physiological Psychology, 72, 51 59. Determinants of social proximity pamine agonists on appetitive and consumma to ry male in Japanese quail (Coturnix coturnix japonica): Male be- sexual behavior in Japanese quail. Neuroscience and Biobehavioral Drug and alcohol consumption and sexual risk behavior Reviews, 13, 1-15. Journal of Comparative and Physiological female rats during estrous cycle, pregnancy and lactation. Effects of endocrine state on sociosexual ior in male rats following lesions of the preoptic-anterior behavior of female rats tested in a complex environment. Sexual motivation: A neural and behavioral ological function of Pavlovian conditioning: A mechanism analysis of the mechanisms underlying appetitive and for mating success in the blue gourami. Studies of instrumental behavior with sexual rein- and castration on sexual behaviour in male rats: studies of forcement in male rats (Rattus norvegicus): I. Control by instrumental behaviour, conditioned place preference and brief visual stimuli paired with a receptive female. D2/D1 ratio in the medial pre- with sexual reinforcement in male rats (Rattus norvegicus): optic area affects copulation of male rats. Effects of preoptic area lesions, castration, and tes to s- macology and Experimental Therapeutics, 251, 422 427. Chronic estradiol quisition of sexual behavior in the male rat: role of female and the facilitation of appetitive sexual behavior in the fe- availability.
Buy phenazopyridine 200 mg visa. Consume Fennel Seeds to Treat Gastritis.
References
- Reyes CN, Wenzel FJ, Lawton BR, Emanuel DA. The pulmonary pathology of farmer's lung disease. Chest 1982;81:142-6.
- Karbe H, Herholz K, Szelies B, et al. Regional metabolic correlates of Token test results in cortical and subcortical left hemispheric infarction. Neurology 1989;39:1083-8.
- Becker M, Marchal F, Becker CD, et al. Sialolithiasis and salivary ductal stenosis: diagnostic accuracy of MR sialography with a three-dimensional extended-phase conjugate-symmetry rapid spin-echo sequence. Radiology 2000;217:347-358.
- Forssell G, Jonasson R, Orinius E. Identifying severe aortic valvular stenosis by bedside examination. Acta Med Scand. 1985;218:397.
- El-Nahas AR, Ibrahim HM, Youssef RF, et al: Flexible ureterorenoscopy versus extracorporeal shock wave lithotripsy for treatment of lower pole stones of 10n20 mm, BJU Int 110(6):898n902, 2012.
- Jordan JE, Zhao ZQ, Sato H, et al: Adenosine A2 receptor activation attenuates reperfusion injury by inhibiting neutrophil accumulation, superoxide generation and coronary endothelial adherence. J Pharmacol Exp Ther 1997;280:301-309.
- Grunberg SM, Osoba D, Hesketh PJ, et al. Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity-an update. Support Care Cancer 2005;13(2);80-84.
- Habazettl H, Conzen PF, Vollmar B, et al: Effect of leukopenia on pulmonary hypertension after heparin-protamine in pigs, J Appl Physiol 73:44, 1992.