
John S. Steinberg, DPM, FACFAS
- Assistant Professor of Plastic Surgery
- Georgetown University Hospital
- Washington, DC
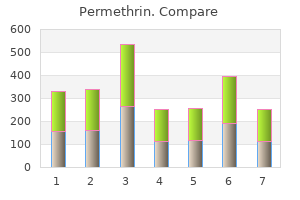
Household treatment Household water treatment technologies are any of a range of devices or methods employed for the purposes of treating water in the home or at the point of use in other settings acne 50 year old woman discount permethrin 30gm online. These are also known as point-of-use or point-of-entry water treatment technologies (Cotruvo & Sobsey acne gel order permethrin line, 2006; Nath skin care brand names buy permethrin 30gm overnight delivery, Bloomfield & Jones acne medication oral cheap permethrin 30gm mastercard, 2006; see also the supporting document Managing water in the home acne zapping machine permethrin 30gm discount, Annex 1) acne zapper cheap permethrin 30gm with mastercard. Household water treatment technologies comprise a range of options that enable individuals and communities to treat collected water or contaminated piped water to remove or inactivate microbial 140 7. Many of these methods are coupled with safe storage of the treated water to preclude or minimize contamination after household treatment (Wright, Gundry & Conroy, 2003). Household water treatment and safe storage have been shown to significantly improve water quality and reduce waterborne infectious disease risks (Fewtrell & Colford, 2004; Clasen et al. Household water treatment approaches have the potential to have rapid and significant positive health impacts in situations where piped water systems are not possible and where people rely on source water that may be contaminated or where stored water becomes contaminated because of unhygienic handling during transport or in the home. Household water treatment can also be used to overcome the widespread problem of microbially unsafe piped water supplies. Similar small technologies can also be used by travellers in areas where the drinkingwater quality is uncertain (see also section 6. Not all household water treatment technologies are highly effective in reducing all classes of waterborne pathogens (bacteria, viruses, protozoa and helminths). For example, chlorine is ineffective for inactivating oocysts of the waterborne protozoan Cryptosporidium, whereas some filtration methods, such as ceramic and cloth or fibre filters, are ineffective in removing enteric viruses. Therefore, careful consideration of the health-based target microbes to control in a drinking-water source is needed when choosing among these technologies. Except for ozone, proper dosing of chemical disinfectants is intended to maintain a residual concentration in the water to provide some protection from post-treatment contamination during storage. Disinfection of household drinking-water in developing countries is done primarily with free chlorine, either in liquid form as hypochlorous acid (commercial household bleach or more dilute sodium hypochlorite solution between 0. This is because these forms of free chlorine are convenient, relatively safe to handle, inexpensive and easy to dose. However, sodium trichloroisocyanurate and chlorine dioxide are also used in some household water treatment technologies. Proper dosing of chlorine for household water treatment is critical in order to provide enough free chlorine to maintain a residual during storage and use. Although these free chlorine doses may lead to chlorine residuals that exceed the recommended chlorine residual for water that is centrally treated at the point of delivery, 0. Disinfection of drinking-water with iodine, which is also a strong oxidant, is generally not recommended for extended use unless the residual concentrations are controlled, because of concerns about adverse effects of excess intake on the thyroid gland; however, this issue is being re-examined, because dietary iodine deficiency is a serious health problem in many parts of the world (see also section 6. As for central treatment, ozone for household water treatment must be generated on site, typically by corona discharge or electrolytically, both of which require electricity. As a result, ozone is not recommended for household water treatment because of the need for a reliable source of electricity to generate it, its complexity of generation and proper dosing in a small application, and its relatively high cost. Strong acids or bases are not recommended as chemical disinfectants for drinking-water, as they are hazardous chemicals that can alter the pH of the water to dangerously low or high levels. However, as an emergency or short-term intervention, the juices of some citrus fruits, such as limes and lemons, can be added to water to inactivate Vibrio cholerae, if enough is added to sufficiently lower the pH of the water (probably to pH less than 4. They rely on physical straining through a single porous surface or multiple surfaces having structured pores to physically remove and retain microbes by size exclusion. Some of these filters may also employ chemical antimicrobial or bacteriostatic surfaces or chemical modifications to cause microbes to become adsorbed to filter media surfaces, to be inactivated or at least to not multiply. Cloth filters, such as those of sari cloth, have been recommended for reducing Vibrio cholerae in water. However, these filters reduce only vibrios associated with copepods, other large crustaceans or other large eukaryotes retained by the cloth. These cloths will not retain dispersed vibrios or other bacteria not associated with copepods, other crustaceans, suspended sediment or large eukaryotes, because the pores of the cloth fabric are much larger than the bacteria, allowing them to pass through. Most household filter technologies operate by gravity fiow or by water pressure provided from a piped supply. However, some forms of ultrafiltration, nanofiltration and reverse osmosis filtration may require a reliable supply of electricity to operate. These filters retain microbes by a combination of physical and chemical processes, including physical straining, sedimentation and adsorption. Some may also employ chemically active antimicrobial or bacteriostatic surfaces or other chemical modifications. Other granular media filters are biologically active because they develop layers of microbes and their associated exopolymers on the surface of or within the granular medium matrix. This biologically active layer, called the schmutzdecke in conventional slow sand filters, retains microbes and often leads to their inactivation and 142 7. A household-scale filter with a biologically active surface layer that can be dosed intermittently with water has been developed. Some use solar radiation to inactivate microbes in either dark or opaque containers by relying on heat from sunlight energy. These may have limited application in developing countries because of the need for a reliable supply of electricity, cost and maintenance requirements. The recommended procedure for water treatment is to raise the temperature so that a rolling boil is achieved, removing the water from the heat and allowing it to cool naturally, and then protecting it from post-treatment contamination during storage. Sedimentation is any method for water treatment using the settling of suspended particles, including microbes, to remove them from the water. These methods may be used along with cloth or fibre media for a straining step to remove the fioc (the large coagulated or precipitated particles that form in the water). This method often employs a series of three pots or other water storage vessels in series, in which sedimented (settled) water is carefully transferred by decanting daily; by the third vessel, the water has been sequentially settled and stored a total of at least 2 days to reduce microbes. These combination treatments include coagulation plus disinfection, media filtration plus disinfection or media filtration plus membrane filtration. When added to water, these chemicals coagulate and fiocculate impurities to promote rapid and efficient sedimentation and also deliver the chemical disinfectant. Other combined treatment technologies are physical devices that include two or more stages of treatment, such as media or membrane filters or adsorbents to physically remove microbes and either chemical disinfectants or another physical treatment process. Many of these combined household water treatment technologies are commercial products that can be purchased for household or other local use. It is important to choose commercial combination devices based on consideration of the treatment technologies that have been included in the device. It is also desirable to require that they meet specific microbial reduction performance criteria and preferably be certified for such performance by a credible national or international authority, such as government or an independent organization representing the private sector that certifies good practice and d ocumented performance. Estimated reductions of waterborne bacteria, viruses and protozoan parasites by several of the above-mentioned household water treatment technologies are summarized in Table 7. These reductions are based on the results of studies reported in the scientific literature. Two categories of effectiveness are reported: baseline removals and maximum removals. Baseline removals are those typically expected in actual field practice when done by relatively unskilled persons who apply the treatment to raw waters of average and varying quality and where there are minimum facilities or supporting instruments to optimize treatment conditions and practices. Maximum removals are those possible when treatment is optimized by skilled operators who are supported with instrumentation and other tools to maintain the highest level of performance in waters of predictable and unchanging quality. It should be noted that there are differences in the log10 reduction value performance of certain water treatment processes as specified for household water treatment in Table 7. These differences in performance by the same treatment technologies are to be expected, because central treatment is often applied to water that is of desirable quality for the treatment process, and treatment is applied by trained operators using properly engineered and operationally controlled processes. In contrast, household water treatment is often applied to waters having a range of water qualities, some of which are suboptimal for best technology performance, and the treatment is often applied without the use of specialized operational controls by people who are relatively untrained and unskilled in treatment operations, compared with people managing central water treatment facilities. Further details on these treatment processes, including the factors that infiuence their performance and the basis for the log10 reduction value performance levels provided in Table 7. The best options for water treatment at the household level will also employ means for safe storage, such as covered, narrow-mouthed vessels with a tap system or spout for dispensing stored water. Validation, surveillance and certification of household water treatment and storage are recommended, just as they are for central water supplies and systems. The entities responsible for these activities for household water treatment systems may differ from those of central supplies. In addition, separate entities may be responsible for validation, independent surveillance and certification. Nevertheless, validation and surveillance as well as certification are critical for effective management of household 146 7. Non-piped water treatment technologies manufactured by or obtained from commercial or other external sources should be certified to meet performance or effectiveness requirements or guidelines, preferably by an independent, accredited certification body. If the treatment technologies are locally made and managed by the household itself, efforts to document effective construction and use and to monitor performance during use are recommended and encouraged. Owing to issues relating to complexity, sensitivity of detection, cost and timeliness of obtaining results, testing for specific pathogens is generally limited to assessing raw water quality as a basis for identifying performance targets and validation, where monitoring is used to determine whether a treatment or other process is effective in removing target organisms. Very occasionally, pathogen testing may be performed to verify that a specific treatment or process has been effective. However, microbial testing included in verification, operational and surveillance monitoring is usually limited to testing for indicator organisms. It is important to recognize that different methods for pathogen detection measure different properties. Culture methods, such as broth cultures or agar-based bacterial media and cell cultures for viruses and phages, detect living organisms based on infection or growth. This creates greater uncertainty regarding the human health risk significance compared with detection by culture-based methods. When using non-culture methods that do not measure in units indicative of culturability or infectivity, assumptions are often made about the fraction of pathogens or components detected that represent viable and infectious organisms. These criteria refiect an assumption that the same organism could be used as an indicator of both faecal pollution and treatment/process efficacy. However, it has become clear that one indicator cannot fulfil these two roles and that a range of organisms should be considered for different purposes (Table 7. For example, heterotrophic bacteria can be used as operational indicators of disinfection effectiveness and distribution system cleanliness; Clostridium perfringens and coliphage can be used to validate the effectiveness of treatment systems. Escherichia coli has traditionally been used to monitor drinking-water quality, and it remains an important parameter in monitoring undertaken as part of verification or surveillance. Water intended for human consumption should contain no faecal indicator organisms. Total coliform bacteria are not acceptable as an indicator of the sanitary quality of water supplies, particularly in tropical areas, where many bacteria of no sanitary significance occur in almost all untreated supplies. Especially under these conditions, medium-term targets for the progressive improvement of water supplies should be set. However, increased attention has focused on the shortcomings of traditional indicators, such as E. Viruses and protozoa more resistant to conventional environmental conditions or treatment technologies, including filtration and disinfection, may be present in treated drinkingwater in the absence of E. Retrospective studies of waterborne disease outbreaks have shown that complete reliance on assumptions surrounding the absence or presence of E. Under certain circumstances, it may be desirable to include more resistant microorganisms, such as bacteriophages and/or bacterial spores, as indicators of persistent microbial hazards. Their inclusion in monitoring programmes, including control and surveillance programmes, should be evaluated in relation to local circumstances and scientific understanding. Such circumstances could include the use of source water known to be contaminated with enteric viruses and parasites or where such contamination is suspected as a result of the impacts of human and livestock waste. Further discussion on indicator organisms is contained in the supporting d ocument Assessing microbial safety of drinking water (Annex 1). The guideline values should be used and interpreted in conjunction with the information contained in these Guidelines and other supporting documentation. A consequence of variable susceptibility to pathogens is that exposure to drinking-water of a particular quality may lead to different health effects in different populations. For derivation of national standards, it is necessary to define reference populations or, in some cases, to focus on specific vulnerable subpopulations. National or local authorities may wish to apply specific characteristics of their populations in deriving national standards. Because the growth medium and the conditions of incubation, as well as the nature and age of the water sample, can infiuence the species isolated and the count, microbiological examinations may have variable accuracy. This means that the standardization of methods and of laboratory procedures is of great importance if criteria for the microbial quality of water are to be uniform in different laboratories and internationally. International standard methods should be evaluated under local circumstances before being adopted. It is desirable that established standard methods be used for routine examinations. It may be necessary to increase disinfection at source, following treatment or during distribution. If microbial quality cannot be maintained, it may be necessary to advise consumers to boil the water during the emergency (see section 7. Initiating superchlorination and undertaking immediate corrective measures may be preferable where the speed of response is sufficient to prevent significant quantities of contaminated water from reaching consumers. During outbreaks of potentially waterborne disease or when faecal contamination of a drinking-water supply is detected, the concentration of free chlorine should be increased to greater than 0. It is most important that decisions are taken in consultation with public health authorities and, where appropriate, civil authorities (see also sections 4.
Which of the listed viewpoints does not belong to the general viewpoints of the implant prosthodontic treatment planfi A) Implant is rigidly fixed in the jaw B) Implant is fixed with a cicatrized tissue in the jaw bone C) It is a histological diagnosis acne on chest permethrin 30 gm visa, according to what the loaded implant and the bone tissue are in contact without an intermediary connective tissue layer D) It is a histological diagnosis skin care jakarta timur order permethrin 30 gm overnight delivery, according to what a connective tissue layer is located between the implant and the bone tissue skin care gift packs buy permethrin online pills. A) the long term formal durability of the implant B) the damage of the implant due to chemical processes C) the damage of the implant due to electrochemical processes D) It is related to the property of the implant which provides the physiological connection with the surrounding tissues skin care di bandung cheap permethrin 30gm on-line. What is the average diameter of the nowadays used cylindrical or screw form implantsfi Restoring a complete maxillary edentulous case acne questionnaire discount permethrin 30gm amex, four implants has been fixed into the frontal part of the edentulous ridge acne 6 days before period discount permethrin 30gm with visa. Which of the following ones does not belong to the inorganic matrix of the bone tissuefi Which jaw bone area can be classified into class D1 according to the Misch and Judy Classificationfi Which of the followings can be listed among the absolute contraindications of implantationfi Which impression tray can be used for the impression taking in case of the use of a transfer abutment, fixed by a transimplant screwfi What kind of prosthetic appliance is indicated in case of complete edentulousness, if there are two implants inserted intraforaminally into the mandibular jawbonefi A free end saddle case is restored with an implant retained fixed prosthetic appliance. Which of the listed ones do not belong to the indication field of the transdental implantationfi Which of the listed ones do belong to the intraoral examinations when planning an implant retained prosthesisfi What is the necessary treatment in the care period of the ready implant prosthesisfi No part of this book may be reproduced in any form or by any means, including photocopying, or utilized by any information storage and retrieval system without written permission from the copyright owner. The publisher is not responsible (as a matter of product liability, negligence, or otherwise) for any injury resulting from any material contained herein. This publication contains information relating to general principles of medical care that should not be construed as specific instructions for individual patients. Printed in China First Edition, 1999 Second Edition, 2003 Third Edition, 2008 Library of Congress Cataloging-in-Publication Data Medicine recall / editor, James D. If they have inadvertently overlooked any, they will be pleased to make the necessary arrangements at the first opportunity. Dedication this book is dedicated to my wife and children, who endured the countless hours I spent with a laptop in front of me. Our challenge in the fourth edition was to update the book to keep pace with the ever-changing field of medicine and to once again be responsive to the valuable feedback by the readers and reviewers. In addition to the update, the goal was for this book to remain portable and therefore, hopefully, useful to the thirdand fourth-year medical students. The author teams for this edition of Medicine Recall were again, in most cases, a medical student, a resident and/or fellow, and an attending for each subspecialty with the idea of framing questions as those posed on rounds. All the sections have been updated and there were continued efforts to shorten the questions and answers as possible. Our hope is that we have once again provided a high-quality product that you will find useful and be able to recommend without reservation to your friends and colleagues. Bergin viii Acknowledgments I acknowledge the hard work of all the authors who contributed to this book. The goal of Medicine Recall is to focus on the diagnosis and treatment of each disease, and Advanced Medicine Recall focuses on the needs of the advanced clerkship students and interns and hones in on the differential diagnosis as well as disease and patient management. The books are organized in a self-study/quiz format with questions on the left side and answers on the right side. It may be worthwhile to cover the right-hand column with the bookmark provided while reading through the book. As in the previous editions of Medicine Recall, the chapters in this guide are organized by systems. When applicable, a list of appropriate landmark clinical trials completes each chapter. The goal is to take all the information gathered from a 45-minute patient interview and exam and distill it down to a 5-minute presentation so that an intelligent plan can be devised to diagnose and treat the patient. A poor or disorganized presentation can make it difficult for anyone to follow and adds unnecessary length and misery to rounds. At the very least organize the material and think about what you are going to say before you start. While presenting on rounds, it is extremely important that you be thoroughly familiar with your patients. As a student, you will not have a large number of patients and, therefore, you should be able to keep all their data. It is fine to refer to your write ups for information about dates, medications, vital signs, etc. The stage is yours without having to fight for attention or trying to upstage any of your colleagues. Make sure you read about the disease(s) your patients have and the studies to be done or proposed. Review your thoughts with your team so that you do not 1 2 Section I / Overview look silly, but make sure you propose a plan of action and why. Also, make lists of problems to be covered while the patient is in so that you are not surprised on the day of discharge. With regard to the team concept, it is extremely important to be thought of as a team player. From an attending standpoint, it is usually easy to recognize people with substantial knowledge and those who want to appear that way. Always lead off with the Chief Complaint and where the information came from and whether it is accurate or suspect. Include all the important past medical problems that relate to the presenting problem. If you are on a subspecialty rotation, adding emphasis to that area would be appropriate. If you are unhappy in your private life, you will likely be unhappy in your professional life as well. This technique also allows the physician to be at the same physical level as the patient, which allows you to talk with and not down to them. Or, alternatively, have all the important physicians present during the critical discussions. Having all important support members present when following up on tests saves repetition and prevents misconceptions that may occur when the information is relayed among those not present. If not all the key players can be present, then realize you will likely need to repeat the information. It is better to take the extra time giving the correct information than to spend the extra time trying to stop the runaway train of misinformation. Because much of the remainder 4 Section I / Overview of the conversation will often be forgotten, it is often best to return to the patient later to review important data. If so, this may be a formidable barrier that may prevent the patient from lifestyle modification. One or more of these should almost always be considered in the differential diagnosis. Drug or food allergies Asthma and anaphylaxis Rhinitis Eczema Urticaria What are the important Any atopic disease including asthma, features of a family historyfi Pulmonary bronchoconstriction (asthma) Pneumonia Pulmonary embolus Pneumothorax Pump failure (congestive heart failure) Pericardial tamponade Psychogenic Poison (carbon monoxide) Peak seekers (high altitude) Paroxysmal spasm of the vocal cords (vocal cord dysfunction) What are important indoor Dust mites, cockroaches, cats, dogs, and allergensfi The specificity of each lymphocyte develops in the absence of antigenic stimulation. Cytokines Cytokines are small proteins produced by activated cells that stimulate different functions, depending on what cells bind them. There are many cytokines in each family (interferons, chemokines, interleukins, etc. Chapter 2 / Allergy and Immunology 7 Antigen An antigen is a protein recognized by the immune system. Idiotypes Idiotypes are unique determinants within the antibody site that recognize antigen. They were first discovered as impediments for transplantation but are crucial to the normal immune response because they are necessary for the presentation of foreign protein to T lymphocytes. The presence of different forms (polymorphisms) is associated with the potential for specific disease states. Adaptive-use gene segments that rearrange somatically to make highly specific antigen-binding molecules List 4 nonspecific 1. What are the final migration Spleen, lymph nodes, intestine, and sites for immature T and B peripheral lymphoid tissue lymphocytesfi What is the function of To facilitate resistance to intracellular T cells (cell-mediated microorganisms. Th1 cytokines activate macrophages and cytolytic T cells and are associated with cell-mediated immunity. What is the function of To mature to plasma cells and produce B cells (humoral immunity)fi What are the 5 major IgA, IgD, IgE, IgG, and IgM classes (isotypes) of immunoglobulinsfi Although IgA is produced in the highest quantities, IgG has higher measurable levels in the blood. It is associated with allergy and with immunity to parasites for which it is thought to assist in antibody-dependent cell cytolysis. It undergoes somatic mutation with affinity maturation, is a potent opsonin (except IgG4), and activates the complement. It is the antigen receptor found on immature B cells and is the first antibody produced in an immune response. Because one form is pentameric (the other is monomeric), activation of complement is strong. Does production of IgM No, production does not require T-cell require the help of T help. What is the basic structure A combination of a heavy chain and a of immunoglobulinsfi Amplification Generation of signals that lead to the release of cytokines that attract other immune components to the site of foreign invasion. Response the stimulating antigen is cleared from the system by effector mechanisms such as infiammation, further innate effector mechanisms. They cause bronchoconstriction, increase mucous secretion, and cause a potent wheal-and-fiare response via increased vascular permeability. Mast cells and basophils are the source of histamine and leukotrienes released in an allergic response. IgE and eosinophils are both produced in response to cytokines expressed by Th2 cells. What proteins are there in Interleukins (so called because they act the cytokine familyfi Opsonizes pathogens, allowing for more efficient phagocytosis, and enhances the clearance of foreign proteins 3. Activates further infiammatory response What activates the classic Immune complexes pathwayfi Generally, which immune IgG and IgM complexes activate the classic complement pathwayfi These fragments generate an infiammatory response by interacting with mast cells, basophils, and other leukocytes and are formed during complement activation.
Generic permethrin 30gm otc. HUGE SKINCARE DECLUTTER + MY HOLY GRAIL SKINCARE PRODUCTS | JuicyJas.
Suicidal gesture as desperate call for help (2) Tricyclic antidepressants have limited 3 skin care chanel buy permethrin 30 gm mastercard. Suicidal ideation and/or gestures with psychosocial and environmental risks such existence of plan requires immediate psychoas impulsivity acne rash buy discount permethrin 30gm, non-conformity/rebellion skin care owned by procter and gamble discount permethrin 30 gm with mastercard, logical evaluation peer pressure acne wash purchase permethrin discount, ineffective coping with stress delex acne buy generic permethrin 30 gm, 3 skin care victoria bc permethrin 30 gm online. Assure safe environment for child/adolescent undiagnosed depression, family dysfunction, including hospitalization if necessary history of child abuse or neglect, parental sub4. Short-term hospitalization is recommended stance abuse for all suicide attempts; attending to emer2. Majority of adolescents will engage in some gency treatment and/or surgical management form of drug use at some point is necessary but insufficient without additional 3. Inform child/adolescent of seriousness of conamong Caucasian teenagers followed by cern and need to notify family and mobilize Hispanic youth; lowest incidence among necessary community resources African-American teenagers a. Identify and provide appropriate referrals for nized and confused thinking, increased management of underlying psychosocial difattention to stimuli; chronic use can ficulties contributing to substance abuse lead to psychosis and major personality 4. Educate and counsel regarding legal and physchanges ical risks of substance abuse b. Support community-based prevention hallucinations; paranoia with aggressive/ programs violent behavior 6. Social recreational use of legal substances development overtime through a variety of 2. Assessment: A more systematic evaluation functioning including suspensions or legal using a standardized or generally accepted difficulties method leading to recommendations for 2. Interviews with and observations from child/ intervention adolescent, parents, school personnel, peers 4. Physical examination with close assessment of abnormality who are correctly identified skin integrity (nasal septum, skin lesions/track through screening (true positives) marks); neurological assessment; vital signs, 5. Specificity: Proportion of those without the weight, height, blood pressure abnormality who are correctly identified as 4. Physical assessment and laboratory screening sentences (refer to chapter 3 on Health Promotion) d. The infiuence of context on development screening tool for toddlers using vocabulary checklist for enumeration 2. Good communication between families, schools, thumb and forefinger that usually is mastered and primary care providers is an example of around: which ecological conceptfi Which of the following findings would be most development of a child who: likely associated with asymmetric intrauterine a. Which developmental theory best explains the misbehaving multifactorial etiology of failure-to-thrivefi Most healthy infants are able to reach, grasp, which parent he prefers living with and hold onto a rattle or other small toy by about: 16. Which of the following strategies would not be not suggest an eating disorder with a purging appropriate to include as part of your managecomponentfi Which of the following situations does not with stress and/or reinforce treatment plan necessarily warrant immediate mental health d. The first physical sign indicating the onset of standing depression but seems to be doing female puberty is: well in school a. A differential diagnosis for child abuse would childhood depression is: include all of the following except: a. The developing person learning disabilities are commonly associated through the life span. Results from the 2005 Identification and evaluation of children with autism National Survey on Drug Use and Health: National spectrum disorders. Assessment tal Health Services Administration Office of Applied of attention deficit hyperactivity disorder: A review Studies. Child maltreatment 2001: Reports from the states Management of children with autism spectrum disto the national child abuse and neglect data system. Evidence-based individualized interventions, on the forefront of promoting and maintaining optiincluding health promotion strategies and mal physical and mental health for children and their anticipatory guidance families. Determine who will be present for interview evidence-based care and individualize interventions, 2. Provide privacy and empathetic environment appropriately involving family members to enhance 3. State you will be taking notes during intermental outcomes in children, adolescents, and their view to enhance accuracy of recorded data families is the implementation of routine child health 5. Use direct questions to obtain specific uration within the context of the family and commuinformation nity. Use language parents and child understand well as specific screening procedures at regular, timed 10. Provide undivided attention; listen carefully, intervals throughout childhood and adolescence. Use projective techniques to elicit information the child and absolutely necessary for the proabout how child is feeling. Some states require reporting of births, deaths, giving detailed information certain diseases, and other vital statistics 5. Communicate with parent first if child is inithe age of 18 years and married, parent of his tially shy or her own child, or self-sufficiently living 2. Ask questions and give explanations using away from home with parental consent) also concrete terminology may sign consents 3. If parent is present, conduct part of interview of minor (questions dealing with personal or sensitive b. Inform older child/adolescent that all questions you are asking have to do with his/her During the examination of a pediatric patient, the hishealth; that you ask all older children/adolestory is critical in the early detection of problems and cents these questions prevention of long-term negative outcomes. Acknowledge that although all of your mately 80% of the information used to arrive at a diagquestions are necessary, some may feel nosis is derived from the history. Inform child that these questions are asked of ties and Peers, Drugs all older school-age children and adolescents 1. Reinforce that although these questions are ily dynamics and relationships, living very personal or sensitive, they are necessary arrangements to gain a complete picture of that child or ado2. Reassure child or adolescent that the informabest and worst subjects, homework, goals, type tion he or she shares is confidential unless of employment and hours worked information about harm to self or others is 3. Make sure older child or adolescent undertory of harm to animals, history of harm to stands meaning of terms used others, Internet use (time, sites, chat rooms, 7. Essential elements of sexual/reproductive personal profiles, e-mail), communication history with strangers, exposure to violence, confiict a. Frequency, length, and quantity of menses membership (self and friends) with associated symptoms;.
X-linked recessive inheritance; carrier detection is possible Thymic Hypoplasia (DiGeorge Syndrome) 2 acne yahoo 30gm permethrin overnight delivery. Frontal bossing coccal vaccines as recommended by the American Academy of Pediatrics; should 6 acne yellow crust buy permethrin 30gm online. Diagnostic findings consistent with -thalassemia be given at least 2 weeks or longer prior to are: surgery acne vulgaris order genuine permethrin line, if possible acne hormonal imbalance buy permethrin 30 gm mastercard, to increase the likelia skin care urdu permethrin 30 gm with mastercard. Which of the following is not included as part problems associated with sickle cell diseasefi Management of a patient with a splenectomy dren: Recommendations from the Advisory Committee does not include: on Childhood Lead Poisoning Prevention acne jaw line purchase permethrin. Primary immunodeficiencies in chilprior to surgery dren: Prompt diagnosis can lead to life-saving treatb. New York: Churchill American Academy of Pediatrics: Subcommittee on HyLivingstone. Inherent dysfunction in transport or assimilation of iodine, or in syntheHypothyroidism sis or metabolism of thyroid hormone. Maternal disease adversely affecting fetal disorder) thyroid development and function (prea. Congenital can cause severe mental natal exposure to iodine-containing or retardation unless treated early; newborn goitrogenic drugs and agents. Iodine deficiency causing endemic goiter of life, usually onset occurs in childhood and cretinism or adolescence. Primary, secondary, tertiary (based on site of pituitary agenesis, anencephaly) disorder) f. Primary disease or disorder of thyroid female to male ratio 2:1 gland (thyroid gland failure) g. Secondary disease or disorder of the American infants pituitary gland that compromises thyroid h. Higher incidence in women, affecting 2% thalamus compromises thyroid gland of women and 0. Absence (athyreosis), underdevelop(more common) and atrophic ment (dysgenesis), of ectopic gland most b. Exposure to iodine-containing drugs and malnutrition; commonly have low T3; normal, agents; drug-induced. Large fontanels, especially posterior; wide permanent or transient disorder sutures, hirsute forehead, coarse facial fea4. Severity, compensated or uncompensated tures, dull expression, facial edema, nasal hypothyroidism refiects the ability to maintain discharge, macroglossia normal T4. Affects multiple systems; many nonspeneck cific, insidious signs and symptoms; severity f. Axillary, prominent supraclavicular fat pads roid deficiency; symptoms vary for infants vs. Distended or protuberant abdomen, diseases; may have maternal prenatal history umbilical hernia, constipation of thyroid disease or ingestion of antithyroid k. Linear growth retardation or growth during first month of life deceleration; delayed bone maturation, b. History of lethargy, poor feeding, prodentition, tooth eruption longed elevated bilirubin (10 mg/dL 3 c. Decreased concentration, memory days of age) impaired, developmental delay, poor c. May be postmature; increased birth motor coordination, dull appearance weight (4000 g) d. History of poor growth, intolerance to disorders cold, poor appetite, constipation. Mental and physical sluggishness, develthickened, increased pigmentation, opmental delay carotenemia f. Possible enlarged thyroid gland (goiter); intrinsic thyroid gland defects from secondary may feel cobblestonelike thyroid deficiency caused by pituitary or hypoh. Newborn screening for congenital hypothyond and third year, and every 4 to 12 months roidism is routine in all 50 states thereafter until growth complete; more frea. Recommended dosages of levothyroxine (T4) tic of transient or permanent primary vary by age; dosage/kg/day decreases over hypothyroidism time with age c. For congenital hypothyroidism, rapid and thyroidism, pituitary tumor) or excess release adequate thyroid hormone replacement of thyroid hormone. Severely affected neonates may have present days or weeks later; not comjaundice, microcephaly, frontal bossmon, but can have severe consequences if ing, craniosynostosis, ophthalmopathy, untreated; diagnosis rarely made in newexophthalmia, thrombocytopenia, cardiac born period problems, hepatosplenomegaly, other b. Prematurity, low birthweight, poor weight signs of severe illness gain, poor feeding 2. Weight loss, although increased apperetraction, stare appearance, periorbital tite; may have accelerated growth and and conjunctival edema advanced bone age with long-term illness c. Nervousness, irritability, decreased attentender, spongy or firm thyroid with tion span, behavior problems, decline in palpable border; may have thyroid bruit or school performance, emotional lability, thrill restlessness, fatigue, weakness, heat intold. Tachycardia, systolic hypertension, erance, increased perspiration increased pulse pressure, palpitations c. Warm, moist, smooth, diaphoretic skin; may have enuresis face may be fiushed; heat intolerance; g. If signs or symptoms of thyrotoxicosis or cotic withdrawal enlarged thyroid, do confirmatory laboratory 2. Although rare in childhood, a child developing ial etiology acute onset of hyperthermia, severe tachycardia, and restlessness needs evaluation for Thyroiditis thyroid crisis or storm 5. Consultation or referral to pediatric endocoxsackie, Epstein-Barr, adenovirus; rare in crinologist for suspected or confirmed U. Prompt diagnosis and treatment especially incidence in children 8 to 15 years; more comimportant in neonates as condition may be mon in females than males (4:1); increasing life-threatening incidence may be associated with rising inci4. Treatment goal is prompt return to euthyroiddence of type 1 diabetes ism with use of: a. With infectious thyroiditis, may have recent propylthiouracil, methimazole history of or concurrent upper respiratory b. Beta-adrenergic receptor blockers to illness control nervousness and cardiovascular 2. Fever, malaise; may feel quite ill with acute or sore throat suppurative or subacute thyroiditis, particud. Ablative therapy with radio-iodine perlarly with former manently suppresses thyroid function; 5. With acute and subacute thyroiditis, pain hypothyroidism induced, but no side and tenderness of thyroid with radiation to effects of medication other areas of neck, ear, chest; with acute supe. Physician consultation or referral to pediatric neck; sensation of tracheal compression endocrinologist for suspected or confirmed 7. Infectious toxic thyroiditis must be disacetylsalicylic acid or other anti-infiammatory tinguished from chronic lymphocytic drugs autoimmune thyroiditis; simple goiters due 3. Benign causes include multinodular increased risk of thyroid microsomal antibody goiter, cysts, follicular adenomas, or 6. Acquired secondary to accidental or surdifferential, elevated sedimentation rate gical trauma, infection, cerebral anoxia, 3. Irritability; may have poor attention span, (2) Electrolyte disorders (hypercalcemia, poor school performance hypokalemia) g. Psychogenic polydipsia (compulsive water normal thirst, diet drinking) and other causes of polyuria. Generally rapid onset; disease may be secondary renal disease; diabetes mellitus) masked as failure to thrive c. Intense thirst, polydipsia, desire for cold unrecognized, infants may have high fever, drinks, preference for cold water; irritable vomiting, seizures, circulatory collapse when fiuid withheld; unable to sleep b. Poor weight gain, deficient growth if long through night without water intake duration, may be malnourished f. Variable levels of dehydration; dry skin, toilet-trained child; clear urine; unable to no tears, no perspiration; if severe, infants concentrate urine after fiuid restriction may have high fever, convulsions, circulai. May have symptoms of intracranial tumor tory collapse (headaches, strabismus, double vision, b. Failure to thrive, malnourished; if long vomiting, precocious puberty) duration, may have growth retardation, j. History of pathological polydipsia and polyweaning (breastmilk has low renal solute uria (2 L/m2/day) in children load), infection, or introduction of solids, 2. Serum osmolality 300 mOsm/kg and pathologic conditions urine osmolality 300 mOsm/kg diagnos2. Genetic counseling may be indicated for familRussell-Silver syndrome; infections; ial etiology placental abnormalities, mater7. History of poor nutritional intake, malablength 50% that of normal child; height sorption syndromes and weight growth deficits; infantile fat b. Short stature associated with bone or deficiency, hypothyroidism, severe systemic cartilage development disorders. Nutritional evaluation may show inadequate ing, abnormal upper to lower body ratios, calories abnormal or disproportionate features, 8. Abnormal home/social evaluation may sugrickets, leg bowing gest psychosocial etiology.
References
- Elstein D, Hollak C, Aerts JM, et al. Sustained therapeutic effects of oral miglustat (Zavesca, N-butyldeoxynojirimycin, OGT 918) in type I Gaucher disease. J Inherit Metab Dis. 2004;27:757-66.
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
- Maiwand MO, Homasson JP. Cryotherapy for tracheobronchial disorders. Clin Chest Med. 1995; 16(3):427-443.
- Ernst AA, Green E, Ferguson MT, et al: The utility of anoscopy and colposcopy in the evaluation of male sexual assault victims. Ann Emerg Med 36:432-437, 2000.
- Yennurajalingam S, Reddy A, Tannir NM, et al. High-dose Asian ginseng (Panax ginseng) for cancer-related fatigue: a preliminary report. Integr Cancer Ther 2015;14(5):419-427.
- Halpern EJ, Verkh L, Forsberg F, et al: Initial experience with contrast-enhanced sonography of the prostate, Am J Roentgenol 174(6):1575n1580, 2000.
- Cho I, Yamanishi S, Cox L, et al. Antibiotics in early life alter the murine colonic microbiome and adiposity. Nature 2012;488(7413):621-626.
- Dumortier P, Coplu L, Broucke I, et al. Erionite bodies and fibres in bronchoalveolar lavage fluid (BALF) of residents from Tuzkoy, Cappadocia, Turkey. Occup Environ Med 2001;58(4):261-6.