
Kathleen Finnegan, MS, MT(ASCP)SHCM
- Clinical Associate Professor
- Chair, Clinical Laboratory Sciences Program
- State University of New York at Stony Brook
- Stony Brook, New York
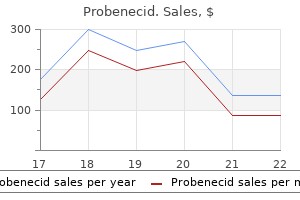
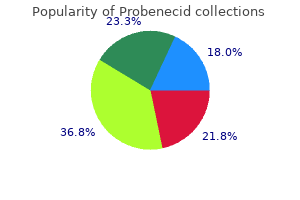
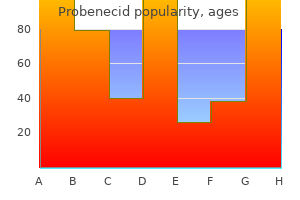
Congenital dyserythropoietic anemia is a rare disorder marked by ineffective erythropoiesis, megaloblastic anemia, and characteristic abnormalities of the nuclear membrane and cytoplasm seen on electron microscopy pain treatment ladder quality probenecid 500mg. This autosomal-recessive disorder is characterized by marrow failure and congenital anomalies, including abnormalities in skin pigmentation, gastrointestinal anomalies, renal anomalies, and upper limb anomalies pain treatment plan cheap probenecid 500 mg overnight delivery. Five genetic phenotypes of Fanconi pancytopenia have been reported, and two of the genes have been cloned wrist pain treatment yahoo discount probenecid online amex. When Fanconi anemia is recognized in a neonate, it is generally on the basis of the congenital anomalies and not the hematologic abnormalities pain treatment consultants of wny probenecid 500mg with mastercard. However, congenital thrombocytopenia, manifested during the immediate newborn period, progressing to pancytopenia has rarely been reported nice guidelines treatment back pain generic 500mg probenecid overnight delivery. A significant percentage of patients develop myelodysplastic syndrome or acute myelogenous leukemia later in life. Treatment of Fanconi pancytopenia includes androgen therapy, and, in many cases, bone marrow transplantation has been successful. Autosomal-recessive osteopetrosis is a rare disorder characterized by osteoclast dysfunction, resulting in a decreased bone marrow space. Patients are generally treated with hematopoietic stem cell transplantation, but they are particularly susceptible to posttransplantation complications after myeloablation, and reduced-intensity conditioning programs may be helpful. Presenting features include failure to thrive, with anemia, neutropenia, and/or thrombocytopenia. The marrow examination typically shows characteristic vacuoles within erythroid and myeloid precursors, hemosiderosis, and ringed sideroblasts. However, risks of transfusions exist and must be weighed against potential benefits each time a transfusion is considered. The idea of sterilely salvaging anticoagulated fetal blood from the umbilical cord and placenta at the time of birth, for a subsequent autologous transfusion for small or sick neonates has had limited study. Reports from Japan182 and Germany183 describe successful cord/ placental blood transfusion for neonates with surgical problems. When oxygen delivery to tissues becomes limited by anemia, oxygen extraction increases and venous oxygen saturation falls. The measurements from each site were averaged into a ratio of oxygen saturations measured from the cerebral and splanchnic sites. Ratios were correlated with independent means of judging whether the transfusion actually provided a benefit. Erythropoietin protects intestinal epithelial barrier function and lowers the incidence of experimental neonatal necrotizing enterocolitis. The biology of erythropoietin in the central nervous system and its neurotrophic and neuroprotective potential. Erythropoietin receptors are expressed in the central nervous system of mid-trimester human fetuses. Erythropoietin and erythropoietin receptor in the developing human central nervous system. Erytropoietin concentrations in cerebrospinal fluid of nonhuman primates and fetal sheep following high-dose recombinant erythropoietin. Erythropoietin and hypoxia inducible factor-1 expression in the mid-trimester human fetus. Reference ranges for hematocrit and blood hemoglobin concentration during the neonatal period: data from a multihospital health care system. Delay clamping of the umbilical cord by 45 to 60 sec after birth, with the neonate in a position lower than the placenta. Strip or milk the umbilical cord at birth, moving additional blood from the placenta and umbilical cord into the neonate, before the umbilical cord is clamped. Develop a consistent approach to minimizing phlebotomy losses in the first days and weeks. Diagnostic laboratory technologies for the fetus and neonate with isoimmunization. Neonatal outcome following long-distance air travel for fetoscopic laser coagulation treatment of twinto-twin transfusion syndrome. Long-term morbidity after fetal endoscopic surgery for severe twin-to-twin transfusion syndrome. Neonatal subgaleal hemorrhage in a multihospital healthcare system: prevalence, associations, and outcomes. Effects of perinatal zidovudine on hematopoiesis: a comparison of effects on progenitors from human fetuses versus mothers. Why, when, and how should we provide red cell transfusions and erythropoiesis-stimulating agents to support red cells mass in neonates Responsiveness to recombinant human erythropoietin of marrow erythroid progenitors from infants with the "anemia of prematurity. Erythroid "burst promoting activity in the serum of patients with the anemia of prematurity. Erythropoietin treatment in extremely low birth weight infants: blood in versus blood out. Late erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Neurodevelopmental outcome and growth at 18 to 22 months corrected age in extremely low birth weight infants treated with early erythropoietin and iron. Recent advances toward defining the benefits and risks of erythrocyte transfusions in neonates. Associations between "early red blood cell transfusion and severe intraventricular hemorrhage, and between "late red blood cell transfusion and necrotizing enterocolitis. The erythrocyte indices of neonates, defined using data from over 12,000 patients in a multihospital health care system. Evaluating neonatal hyperbilirubinemia in late preterm Hispanic twins led to the diagnosis of hereditary spherocytosis in them, and in their sibling and in their mother. Reference ranges for blood concentrations of nucleated red blood cells in neonates. Reference ranges for lymphocyte counts of neonates: associations between abnormal counts and outcomes. Hematocrit correlates well with circulating red blood cell volume in very low birth weight infants. The effect of early and late cordclamping on blood viscosity and other hemorheological parameters in fullterm neonates. Delayed cord clamping in very preterm infants reduces the incidence of intraventricular hemorrhage and late-onset sepsis: a randomized, controlled trial. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks gestation: a randomised controlled trial. Molecular defect of spectrin in a subset of patients with hereditary elliptocytosis. Cord blood red cell osmotic fragility: a comparison between preterm and full-term newborn infants. Isoelectric focusing of hexokinase and glucose-6-phosphate dehydrogenase isoenzymes in erythrocytes of newborn infants and adults. Use of erythropoietin and its effects on blood lactate and 2, 3-diphosphoglycerate in premature neonates. Different effects of 2,3-diphosphoglycerate and adenosine triphosphate on oxygen affinity of adult and fetal human hemoglobin. Postnatal changes in oxygen transport of term, premature, and sick infants: the role of red cell 2,3-diphosphoglycerate and adult hemoglobin. Transfusion-related acute gut injury: necrotizing enterocolitis in very low birth weight neonates after packed red blood cell transfusion. Is "transfusion-associated necrotizing enterocolitis an authentic pathogenic entity Do red cell transfusions increase the risk of necrotizing enterocolitis in premature infants A clinical study on the feasibility of autologous cord blood transfusion for anemia of prematurity. A randomized clinical trial comparing immediate versus delayed clamping of the umbilical cord in preterm infants: short-term clinical and laboratory endpoints. Potential use of autologous umbilical cord blood red blood cells for early transfusion needs of premature infants. Is there a role for autologous/placental red blood cell transfusions in the anemia of prematurity Cerebral tissue oxygen saturation and extraction in preterm infants before and after blood transfusion. Blood transfusions increase cerebral, splanchnic, and renal oxygenation in anemic preterm infants. Packed red blood cell transfusion increases regional cerebral and splanchnic tissue oxygen saturation in anemic symptomatic preterm infants. Splanchnic-cerebral oxygenation ratio as a marker of preterm infant blood transfusion needs. Polycythemia ("many cells") describes an increase in the total quantity or volume (mass) of red blood cells in the body without any implication regarding leukocytes or platelets. Erythrocytosis may be the result of an increase in the red cell volume or mass (polycythemia; also called absolute erythrocytosis) or the result of a reduced plasma volume (called relative or spurious polycythemia or erythrocytosis), which produces an increase in red cell concentration that does not reflect an increase in the quantity of red cells in the body. Despite the precision with which these terms are defined, opportunities for confusion abound. Polycythemia vera (also called polycythemia rubravera) is a myeloproliferative disorder associated with trilineage marrow hyperplasia and characterized by an increased red cell mass, usually in association with leukocytosis and thrombocytosis. Some patients who do not have this myeloproliferative disease are described as having polycythemia vera simply because they have an elevated red cell mass. Confusion on this point is frequently encountered in consultative hematology practice. This section focuses primarily on the contribution of red cell concentration to viscosity and oxygen transport; more complete discussions are available elsewhere. As the red cell mass rises, the total blood volume typically increases: the variability of changes in plasma volume means that the degree of increase is unpredictable. In addition, the increased blood volume and increased blood viscosity that occur in association with polycythemia themselves produce certain symptoms and signs; these are related to the degree of the increase and the resulting effects on blood flow and oxygen transport. Blood Viscosity and Oxygen Transport Viscosity is an intrinsic characteristic of a liquid and represents the tendency of that liquid to resist changes in shape. Relation of volume of packed red cells (hematocrit) to blood viscosity in centipoise (cp) as measured in a capillary viscosimeter compared with that calculated for shear rates of 120 sec-1 (ascending aorta) and 12 sec-1 (medium arteriole). It is noted above that the model for determining blood viscosity represents a somewhat artificial system: calculated values probably exceed those existing in vivo. Hematocrit reduction, either by venesection18,19,20,21 or by volume expansion,21 improved cerebral blood flow. The determination of blood viscosity values at different hematocrits allows the estimation of blood flow rates under different conditions. At a given vessel size and pressure gradient, the predicted relation of oxygen transport to hematocrit is expressed by an arch-shaped curve. Optimal oxygen transport would be predicted to occur in the normal hematocrit range. In polycythemia, the associated hypervolemia permits an oxygen transport curve that is similar to that of normovolemic patients but which is elevated and shifted to the right. In contrast, in patients who have a normal or decreased total blood volume (as in relative or spurious polycythemia), erythrocytosis has an adverse effect on oxygen transport. Arterial oxygen transport at different volumes of packed red cells and thus different viscosity values. A: Values in curve were calculated from blood viscosity values as measured by Pirofsky. The circulatory effects of hematocrit variations in normovolemic and hypovolemic dogs. Patients with polycythemia vera have no need for increased tissue oxygen transport. When treating by phlebotomy, however, blood volume should not be reduced too greatly at any one episode, especially in patients with known symptoms of cardiovascular disease (angina pectoris, transient ischemic attacks). This is particularly true early in the course of therapy, when hematocrit (and consequently viscosity) is highest. Another concern is that a sudden fall in blood volume from any cause, such as dehydration or acute hemorrhage, may result in local ischemia because increased cardiac output cannot compensate immediately for the effects of high viscosity. In patients with congestive heart failure, the need for reduction of blood viscosity may be urgent, because the ability to increase cardiac output to compensate for the increased blood viscosity has been compromised. The secondary polycythemic syndromes are divided into those that represent a response to tissue hypoxia (physiologically appropriate) and those driven by erythropoietin not produced in response to tissue hypoxia (physiologically inappropriate). Although actual polycythemia can usually be differentiated from relative polycythemia on clinical grounds (as described below), an assessment of the red cell mass is the initial step in evaluation. Traditionally, this has been done by measurement of red cell mass and blood volume by isotope labeling. It has been proposed that a red cell mass of at least 125% of that predicted should be considered as indicating polycythemia. In the view of most,36,37,38 but not all,15 investigators, this practice is associated with an increased chance of error; measuring red cell mass and plasma volume separately is preferable. It must be emphasized that blood volume measurements do not differentiate between secondary polycythemia and polycythemia vera; they are useful only in distinguishing absolute from relative erythrocytosis. However, availability of actual red cell volume measurement has become limited to a small number of large medical centers with special expertise. Surrogate measures based on Hb or hematocrit are now the routine basis for distinguishing relative and actual polycythemia. Such patients typically exhibit anasarca and other physical findings suggestive of severe intravascular volume depletion and redistribution of intravascular volume. The characteristics of polycythemia vera are outlined in Chapter 82; the other polycythemic syndromes are discussed below.
Methemoglobin occurs when the ferrous molecule is oxidized to ferric (Fe3+), either in the usual course of events quadriceps pain treatment buy probenecid without a prescription. Methemoglobin causes two sorts of problems: methemoglobin cannot bind oxygen, and, further, if a methemoglobin becomes part of the hemoglobin tetramer, the oxygen affinity is increased with a left shift in the oxyhemoglobin dissociation curve and a biologically important fall in the partial pressure of oxygen at which hemoglobin is 50% saturated with oxygen (P50) back pain treatment vibration purchase 500mg probenecid otc. Methemoglobin is being formed continuously, but there are mechanisms in place that normally keep the methemoglobin level at about 1% of the total hemoglobin pain treatment center houston tx purchase probenecid 500mg without prescription. Two molecules of ferric (Fe3+) cytochrome b5 are then sequentially bound and reduced, forming ferrous (Fe2+) cytochrome b5 wrist pain yoga treatment cheap probenecid 500 mg mastercard. An ionic complex between ferrous (Fe2+) cytochrome b5 and a ferric (Fe3+) subunit of a hemoglobin (methemoglobin) tetramer is formed and an electron transferred between the two hemes, creating ferrous (Fe2+) hemoglobin pain home treatment purchase probenecid 500 mg with amex. When oxygen is bound, an electron is partially transferred from the iron moiety to the bound oxygen, forming a ferric-superoxide anion complex (Fe3+-O2-). The partially transferred electron is not returned to the iron moiety, leaving the iron in the ferric state (Fe3+) and forming methemoglobin (metHb). Chapter 42 Red Blood Cell Enzymopathies 589 Substances Associated With Methemoglobinemia Acetaminophen (nitrobenzene derivative) Acetanilide Local anesthetics Benzocaine Lidocaine Prilocaine Aniline dyes Celecoxib Dapsone Flutamide Ifosfamide Metoclopramide Nitric oxide Nitrites Amyl nitrite Isobutyl nitrite Sodium nitrite Nitrates (bacterial conversion to nitrites) Nitrobenzenes/nitrobenzoates Nitroethane (nail polish remover) Nitrofurans Nitroglycerin Paraquat/monolinuron Phenacetin Phenazopyridine (Pyridium) Primaquine Rasburicase Sulfamethoxazole Laboratory Manifestations and Diagnosis Methemoglobinemia should be suspected when the patient appears cyanotic but has a normal PaO2 as measured by arterial blood gas assessment. The blood will typically be a dark purple to chocolate color, and the blood will not become more red on exposure to oxygen. Pulse oximetry is unreliable in the presence of methemoglobinemia, due to its light absorbance properties198; however, cooximetry can determine the methemoglobin fraction. In the case of acute onset due to oxidizing agents or disease states, any potential offending agents should be immediately discontinued. The asymptomatic patient with methemoglobin levels of less than 20% may only need observation. If the patient is symptomatic or if methemoglobin levels are greater than 20%, intervention with methylene blue is indicated. Methylene blue is given in a dose of 1 to 2 mg/kg intravenously over 5 minutes, and the dose may be repeated after 60 minutes if necessary. Cumulative doses greater than 4 to 7 mg/kg (or even lower in infants) may cause cyanosis, dyspnea, and acute hemolysis. Neonates are at particularly increased risk due to decreased Cb5R activity (50% to 60% of adult activity). Hereditary Methemoglobinemia Hereditary causes of methemoglobinemia are secondary to deficiency of Cb5R, very rarely described deficiency of cytochrome b5,207 or inheritance of an abnormal hemoglobin in hemoglobin M disease (see Chapter 41). Cytochrome-b5 Reductase Deficiency Cb5R deficiency is the most common cause of congenital methemoglobinemia and is inherited in an autosomal recessive manner. This is the more common form of hereditary methemoglobinemia and is endemic in certain populations, including Navajo211 and Athabasca212 Native Americans and natives of Yakutsk, Siberia. The cyanosis can be treated with oral doses Clinical Manifestations Clinical manifestations develop secondary to impaired tissue oxygenation. Typical "cyanotic" slate-blue coloring of the skin and mucous membranes will be visible when 5% to 15% of the total hemoglobin is methemoglobin. The onset of disease may be abrupt, and the clinician must maintain a high index of suspicion in at-risk situations. The mutation was determined to be a missense mutation near the active binding site of the enzyme. These patients may, however, be more sensitive to decreases in hemoglobin and become symptomatic from what would otherwise be deemed a mild anemia. Baronciani L, Beutler E: Molecular study of pyruvate kinase deficient patients with hereditary nonspherocytic hemolytic anemia. Beutler E: Glucose-6-phosphate dehydrogenase deficiency: A historical perspective. It binds to a central cavity of the hemoglobin tetramer and allosterically converts hemoglobin to a low oxygen affinity state, resulting in a rightward shift of the oxygen dissociation curve. The ensuing increase in hemoglobin oxygen affinity results in a decrease in oxygen delivery to the tissues, which in turn leads to a compensatory polycythemia. Due to the rarity of the condition, there is limited experience to guide treatment. Presumably the reactive polycythemia compensates for the diminished oxygen delivery to the tissues and thereby Chapter 42 Red Blood Cell Enzymopathies 591 Kaplan M, Hammerman C: the need for neonatal glucose-6-phosphate dehydrogenase screening: A global perspective. Youngster I, Arcavi L, Schechmaster R, et al: Medications and glucose-6phosphate dehydrogenase deficiency: An evidence-based review. Zaffanello M, Rugolotto S, Zamboni G, et al: Neonatal screening for glucose6-phosphate dehydrogenase deficiency fails to detect heterozygote females. Zanella A, Bianchi P, Fermo E, et al: Hereditary pyrimidine 5-nucleotidase deficiency: From genetics to clinical manifestations. Zanella A, Fermo E, Bianchi P, et al: Pyruvate kinase deficiency: the genotypephenotype association. The natural course of the hemolytic anemia and the mechanism of its self-limited character. Beutler E: the glutathione instability of drug-sensitive red cells: A new method for the in vitro detection of drug sensitivity. Beutler E, Robson M, Buttenwieser E: the mechanism of glutathione destruction and protection in drug-sensitive and non-sensitive erythrocytes: In vitro studies. Atamna H, Pascarmona G, Ginsburg H: Hexose-monophosphate shunt activity in intact Plasmodium falciparum-infected erythrocytes and in free parasites. Luzzatto L, Sodeinde O, Martini G: Genetic variation in the host and adaptive phenomena in Plasmodium falciparum infection. Shalev O, Wollner A, Menczel J: Diabetic ketoacidosis does not precipitate haemolysis in patients with the Mediterranean variant of glucose-6-phosphate dehydrogenase deficiency. Schiliro G, Russo A, Curreri R, et al: Glucose-6-phosphate dehydrogenase deficiency in Sicily. Kaplan M, Hammerman C: Glucose-6-phosphate dehydrogenase deficiency: A hidden risk for kernicterus. Valaes T: Pathophysiology of spontaneous neonatal bilirubinemia associated with glucose-6-phosphate dehydrogenase deficiency. Kaplan M, Renbaum P, Levy-Lahad E, et al: Gilbert syndrome and glucose-6-phosphate dehydrogenase deficiency: A dose-dependent genetic interaction crucial to neonatal hyperbilirubinemia. Beutler E: A series of new screening procedures for pyruvate kinase deficiency, glucose-6-phosphate dehydrogenase deficiency, and glutathione reductase deficiency. Zaffanello M, Rugolotto S, Zamboni G, et al: Neonatal screening for glucose-6-phosphate dehydrogenase deficiency fails to detect heterozygote females. Youngster I, Arcavi L, Schechmaster R, et al: Medications and glucose6-phosphate dehydrogenase deficiency: An evidence-based review. Kaplan M, Hammerman C: Glucose-6-phosphate dehydrogenasedeficient neonates: A potential cause for concern in North America. Sgro M, Campbell D, Shah V: Incidence and causes of severe neonatal hyperbilirubinemia in Canada. Beutler E, Gelbart T, Kondo T, et al: the molecular basis of a case of gamma-glutamylcysteine synthetase deficiency. Hirono A, Iyori H, Sekine I, et al: Three cases of hereditary nonspherocytic hemolytic anemia associated with red blood cell glutathione deficiency. Ristoff E, Mayatepek E, Larsson A: Long-term clinical outcome in patients with glutathione synthetase deficiency. Ristoff E, Hebert C, Njalsson R, et al: Glutathione synthetase deficiency: Is gamma-glutamylcysteine accumulation a way to cope with oxidative stress in cells with insufficient levels of glutathione Loos H, Roos D, Weening R, et al: Familial deficiency of glutathione reductase in human blood cells. Boivin P, Galand C, Hakim J, et al: [Hemolytic anemia with glutathione peroxidase deficiency in an adult]. Nishimura Y, Chida N, Hayashi T, et al: Homozygous glutathioneperoxidase deficiency of erythrocytes and leukocytes. Beutler E, Matsumoto F: Ethnic variation in red cell glutathione peroxidase activity. Beutler E, Gelbart T: Estimating the prevalence of pyruvate kinase deficiency from the gene frequency in the general white population. Hirono A, Forman L, Beutler E: Enzymatic diagnosis in non-spherocytic hemolytic anemia. Lenzner C, Nurnberg P, Jacobasch G, et al: Molecular analysis of 29 pyruvate kinase-deficient patients from central Europe with hereditary hemolytic anemia. Pastore L, Della Morte R, Frisso G, et al: Novel mutations and structural implications in R-type pyruvate kinase-deficient patients from Southern Italy. Zanella A, Fermo E, Bianchi P, et al: Pyruvate kinase deficiency: the genotype-phenotype association. Noguchi T, Yamada K, Inoue H, et al: the L- and R-type isozymes of rat pyruvate kinase are produced from a single gene by use of different promoters. Takegawa S, Fujii H, Miwa S: Change of pyruvate kinase isozymes from M2- to L-type during development of the red cell. Ishida Y, Miwa S, Fujii H, et al: Thirteen cases of pyruvate kinase deficiency found in Japan. Aizawa S, Kohdera U, Hiramoto M, et al: Ineffective erythropoiesis in the spleen of a patient with pyruvate kinase deficiency. Aizawa S, Harada T, Kanbe E, et al: Ineffective erythropoiesis in mutant mice with deficient pyruvate kinase activity. Ferreira P, Morais L, Costa R, et al: Hydrops fetalis associated with erythrocyte pyruvate kinase deficiency. Zanella A, Fermo E, Bianchi P, et al: Red cell pyruvate kinase deficiency: Molecular and clinical aspects. Paravertebral extramedullary haemopoiesis associated with pyruvate kinase deficiency. Bachmeyer C, Khalil A, Kerrou K, et al: Idiopathic pulmonary arterial hypertension in a patient with pyruvate kinase deficiency and paravertebral extramedullary hematopoiesis. Hilgard P, Gerken G: Liver cirrhosis as a consequence of iron overload caused by hereditary nonspherocytic hemolytic anemia. Lopez C, Saravia C, Gomez A, et al: Mechanisms of genetically-based resistance to malaria. Perseu L, Giagu N, Satta S, et al: Red cell pyruvate kinase deficiency in Southern Sardinia. Sandoval C, Stringel G, Weisberger J, et al: Failure of partial splenectomy to ameliorate the anemia of pyruvate kinase deficiency. Garcia M, Pujol A, Ruzo A, et al: Phosphofructo-1-kinase deficiency leads to a severe cardiac and hematological disorder in addition to skeletal muscle glycogenosis. Nakajima H, Raben N, Hamaguchi T, et al: Phosphofructokinase deficiency: Past, present and future. Serdaroglu G, Aydinok Y, Yilmaz S, et al: Triosephosphate isomerase deficiency: A patient with Val231Met mutation. Zanella A, Bianchi P, Fermo E: Hereditary pyrimidine 5-nucleotidase deficiency: From genetics to clinical manifestations. Kanno H, Takizawa T, Miwa S, et al: Molecular basis of Japanese variants of pyrimidine 5-nucleotidase deficiency. Bianchi P, Fermo E, Alfinito F, et al: Molecular characterization of six unrelated Italian patients affected by pyrimidine 5-nucleotidase deficiency. David O, Ramenghi U, Camaschella C, et al: Inhibition of hexose monophosphate shunt in young erythrocytes by pyrimidine nucleotides in hereditary pyrimidine 5 nucleotidase deficiency. Rechavi G, Vonsover A, Manor Y, et al: Aplastic crisis due to human B19 parvovirus infection in red cell pyrimidine-5-nucleotidase deficiency. Dvilansky A, Hezkelson L, Wolfson M, et al: Haemolytic anaemia due to pyrimidine-5-nucleotidase deficiency. Darling R, Roughton F: the effect of methemoglobin on the equilibrium between oxygen and hemoglobin. Comparative studies of diaphorases from normal and methemoglobinemic erythrocytes. Public Health Advisory: Benzocaine sprays marketed under different names, including Hurricaine, Topex and Cetacaine. Guay J: Methemoglobinemia related to local anesthetics: A summary of 242 episodes. Methylene blue induced cyanosis and acute hemolytic anemia complicating the treatment of methemoglobinemia. Perera M, Shihana F, Kularathne K, et al: Acute methaemoglobinaemia after massive nitrobenzene ingestion. Lindenmann J, Matzi V, Kaufmann P, et al: Hyperbaric oxygenation in the treatment of life-threatening isobutyl nitrite-induced methemoglobinemia-a case report. Hegesh E, Hegesh J, Kaftory A: Congenital methemoglobinemia with a deficiency of cytochrome b5. Gallagher Characterization of the structure and function of red blood cell membrane proteins and their genes. Likewise, knowledge of the molecular mechanisms underlying changes in red blood cell deformability, structural integrity, and shape has advanced. Red blood cell shape abnormalities often provide a clue to the pathobiology and diagnosis of the underlying disorder. Vertical interactions, which are perpendicular to the plane of the membrane, stabilize the lipid bilayer. Horizontal interactions, which are parallel to the plane of the membrane, support the structural integrity of erythrocytes after their exposure to shear stress. Horizontal interactions involve the spectrin heterodimer association site, where spectrin heterodimers assemble into tetramers, the principal building blocks of the membrane skeleton, and the contacts of the distal ends of spectrin heterodimers with actin and protein 4. Although interactions between proteins of the erythrocyte membrane are significantly more complex than can be classified by this model of horizontal and vertical interactions, the model serves as a useful starting place for understanding erythrocyte membrane protein interactions, particularly in reference to membrane-related disorders. Consequently the lipid bilayer membrane is destabilized, leading to release of bilayer lipids from the cells in the form of skeleton-free lipid vesicles.
If patients do not display at least a partial response within 2 to 3 weeks of therapy initiation, salvage therapy should be considered pain treatment center llc 500mg probenecid overnight delivery. Recurrence of fever and increased inflammatory markers after an apparent response should also prompt a careful search for opportunistic infection advanced pain treatment center union sc purchase probenecid paypal. Changes in mental status at any time during therapy should be investigated urgently sciatica pain treatment natural effective 500mg probenecid. Because of its immunoablative qualities, alemtuzumab should be used with caution and by those with experience caring for profoundly immune compromised patients chiropractic treatment for shingles pain buy probenecid with paypal. In contrast to refractory patients, those patients who initially respond well to standard therapy but then relapse as treatment is tapered or withdrawn often respond to reintensification of therapy with standard agents pain treatment with laser cheap 500 mg probenecid free shipping. Because of inflammation, consumptive coagulopathy, and intrinsic platelet defects in some patients, they are at very high risk of spontaneous bleeding. Most patients transplanted during that era succumbed to "transplant-related" complications during the first 100 days after infusion. The timing of pretransplant alemtuzumab impacts the probability of graft-versus-host disease; mixed chimerism; and in rare cases, rejection. Cyclosporine may be added in patients with stable blood pressure and adequate liver and kidney function. Notably, most deaths occurred during the first few weeks of treatment and may reflect either preexisting morbidities or primary refractory disease. Patients with significant neurologic involvement may experience severe and permanent sequelae even if they survive. Alternative strategies using anticytokine antibodies for induction therapy are also being developed. In the foreseeable future, a variety of new, rationally designed immunosuppressive agents are likely to come into clinical use for transplantation and autoimmune disorders. Future studies will likely focus on defining which sort of immune suppression displays the best balance of safety and efficacy. Early recognition of this syndrome and immediate therapeutic intervention to produce a rapid response are critical. Prompt administration of more aggressive treatment in these patients may, in fact, prevent development of the full-blown syndrome. To achieve rapid reversal of coagulation abnormalities and cytopenias, most clinicians start with intravenous methylprednisolone pulse therapy (30 mg/kg for 3 consecutive days) followed by 2 to 3 mg/kg/day divided in four doses. The upper respiratory mucosa is involved in 20% of patients, bone in 25%, and orbit or eyelid in 10%. Eighty percent of patients are diagnosed in the first or second decade of life; however, the disorder also can affect elderly adults. A characteristic finding, referred to as emperipolesis, demonstrates lymphocytes surrounded by the membranes of histiocytes as observed best by electron microscopy. The etiology of Rosai-Dorfman disease is unknown, but disordered immune regulation has been proposed as a significant contributor. It was originally thought that Rosai-Dorfman disease represented an unusual response to herpesviruses, but this has not been confirmed. Although patients frequently are febrile, infectious agents are not commonly implicated, and the fever is presumed to be a manifestation of systemic disease. Five died of "immunologic" causes, such as severe hemolysis; three died of infections; and six probably died as a direct consequence of disease infiltration. Corticosteroids, vinblastine, and low-dose cyclophosphamide are sometimes effective; however, the results with these agents have been inconsistent. Attempts at treatment should be reserved for special circumstances, such as tracheal or epidural compression or invasion of other vital structures, as well as for significant cosmetic disfigurement. Local excision may be useful in selected patients, although the lesions may reappear. Arnaud L, Gorochov G, Charlotte F, et al: Systemic perturbation of cytokine and chemokine networks in Erdheim-Chester disease: A single-center series of 37 patients. Fahrner B, Prosch H, Minkov M, et al: Long-term outcome of hypothalamic pituitary tumors in Langerhans cell histiocytosis. Minkov, M: Multisystem Langerhans cell histiocytosis in children: Current treatment and future directions. Weitzman, S, Jaffe R: Uncommon histiocytic disorders: the non-Langerhans cell histiocytoses. Originally described by DeDuve and colleagues,1 lysosomes are ubiquitous organelles required to metabolize macromolecules. This includes molecules internalized by cells through the process of endocytosis, as well as those produced during the natural turnover of endogenous cell components (autophagocytosis). More than 50 hydrolytic enzymes have been found within the lysosome, as well as several membrane-embedded transport proteins, ion pumps, and other specialized components. Unique to the lysosome is a highly acidic pH, and the enzymes and proteins found within this organelle have evolved to optimally function within this unique environment. To date, more than 50 disorders have been attributed to defective lysosomal proteins. The pathophysiology of these diseases is directly related to these accumulating material(s), although as the diseases progress many secondary abnormalities also occur and contribute to the disease pathology. There is also considerable cell and organ specificity related to the location and function of the specific macromolecules affected. At this stage, all proteins destined for the lysosomes contain only branched mannosyl oligosaccharide chains that terminate with short-chain -glucosyl moieites. During transport through the Golgi apparatus, they acquire additional, complex oligosaccharide modifications that result in their sorting to lysosomes. A series of glycosyl hydrolases and transferases within specific regions of the cis-, mid-, and trans-Golgi participate in these sequential modifications. For example, in the cis-Golgi, -glucosidase and -mannosidases remove terminal glucose and mannose residues to produce mannose-terminated core oligosaccharides. Within the mid-Golgi, additional sugars are added, including -N-acetylglucosamine and -galactoside. Coincident with the addition of the -N-acetylglucosamine moiety is the addition of a phosphate group to this sugar by the enzyme N-acetylglucosaminyl-1-phosphotransferase. In the Golgi apparatus, the carbohydrate chains are modified to acquire M6P residues, allowing sorting of these proteins to newly formed lysosomes by interaction with M6P receptors embedded in the membrane. Interaction of the M6P-containing proteins with the receptors occurs in the trans-Golgi, where the newly formed vesicles bud from the Golgi membrane and undergo sequential acidification to become mature lysosomes. These vesicles also may fuse with endosomal vesicles that deliver materials from the cell surface. Two enzymes localized in the Golgi are responsible for the creation of the M6P residues, and a deficiency of one can lead to a rare inherited disorder (I-cell disease) in which many of the lysosomal proteins are abnormally sorted and secreted from cells. Within the mature acidified lysosomes, additional proteolytic and carbohydrate modifications may occur, leading to full activity of the proteins. Acidification also triggers the release of the M6P-containing proteins from the receptors. In addition, within lysosomes, the active and mature proteins may associate into higher order molecular scaffolds that function to degrade the macromolecules. Central to the formation of a mature lysosome is the establishment of an acidic pH. Mature lysosomes have a pH below 5, which is maintained by a proton pump found within the lysosomal membrane. Acidification of the compartment is required for proper activation of the hydrolytic enzymes and the release of macromolecules from their membrane receptors, providing access to the fully active hydrolytic enzymes. Although lysosomes have been historically considered discrete organelles, it is now known that the lysosomal system is highly dynamic and consists of a series of digestive vesicles with varying pH, hydrolytic enzyme activities, and cellular location. This is accomplished through a series of specific targeting mechanisms unique to these proteins4 (see box on Lysosomal Protein Biosynthesis and Sorting). Importantly, for any given lysosomal enzyme, the oligosaccharide chains may be highly heterogeneous, containing varying amounts of M6P, sialic acid, and glucosaminyl sugars. In addition to targeting the lysosomal enzymes to the organelle, the oligosaccharide side chains also participate in the tertiary structure and folding of the proteins and are in many cases necessary for their activity. Proteolytic processing within the lysosome is also sometimes required for activity, as well as assembly into macromolecular "scaffolds" that may include protector proteins, activators, and so on. Finally, although most lysosomal enzymes use the M6P targeting system, it is also important to recognize that non-M6P targeting systems have been described and may function alone or in combination with M6P. A small number of the diseases also result from mutations in genes encoding defective transport proteins that reside within the lysosomal membrane or other nonhydrolytic enzymes required for lysosomal enzyme biosynthesis. For example, progressive lysosomal accumulation of glycosphingolipids in the central nervous system leads to neurodegeneration, and storage in visceral cells can lead to organomegaly, skeletal abnormalities, pulmonary infiltration, and other manifestations. The accumulation of these materials results in severe cartilage and bone abnormalities that affect the skeletal system, trachea, and other organs, which are characteristic of the disorders. Globosides, in particular, are synthesized in visceral tissues, resulting in visceral storage in Sandhoff disease. In addition, because most lysosomal enzymes are likely assembled in higher order molecular scaffolds in which their activities are tightly and coordinately controlled, this also likely contributes to the multiple effects of the single enzyme deficiencies. As the macromolecules accumulate, the lysosomes become distended and destabilized and eventually may fail to carry out their normal functions related to phago- and autophagocytosis. In turn, this may result in cell senescence or death or at the very least cell dysfunction. However, because the inflammatory cells themselves are dysfunctional, the diseases progress, and the inflammatory changes may become chronic. The genes encoding most lysosomal proteins have been cloned, and there is no obvious clustering of these genes within the genome. In some cases, nonfunctional pseudogenes also have been described, which may or may not be transcribed or translated into a nonfunctional protein. However, because the newly formed lysosomes in these diseases will retain the same primary metabolic defect, this may lead to amplification of the disease pathology. In general, heterozygous "carriers" of single mutations in a lysosomal gene do not develop clinical symptoms of the disorder, except in the X-linked disorders (Fabry and Hunter diseases), where X-inactivation patterns can lead to clusters of cells without enzyme activity that develop disease related pathology. For some disorders, carrier identification and prenatal diagnosis are available as well. However, because the detection of individual enzyme activities in these cell sources must use in vitro assay conditions and nonnatural substrate analogues. For this reason, predicting the clinical outcome from these analyses is generally not reliable. For most diseases, multiple mutations have been found, and the majority of these are unique. Such individuals are referred for genetic counseling to assist with family planning and pregnancy outcome choices. The implication of such screening has led to a dramatic reduction in the incidence of some diseases within this population. This can be accomplished by stem cell transplantation, protein replacement therapy, or gene therapy. In some cases, treatments also have been developed that are either aimed at slowing the accumulation of undegraded materials (substrate reduction therapy) or enhancement of the mutant protein function (chaperone therapy). The premise of this approach is that stem cells in the bone marrow will repopulate in the transplanted individual and provide a source of secreted and normal lysosomal proteins that can be taken up by neighboring cells for metabolic correction (cross-correction). However, despite the availability of cord blood registries, such cell transplantation is still limited by a high morbidity and the lack of suitable donors. This approach, although effective, requires lifelong weekly or biweekly infusions of the recombinant proteins, and the costs are very high. This approach, however, has also proven very effective in some disease models and could be evaluated in the clinic during the upcoming years. In general, the efficacy of any of these approaches is dependent on the cellular and tissue sites of pathology and the ability of the therapeutic proteins, stem cells, or gene therapy vectors to access these sites. The premise of this approach is that transplanted cells expressing the normal lysosomal proteins would release some of these proteins into the circulation and locally at the sites of pathology and that these proteins would be taken up by the diseased cells, leading to metabolic "crosscorrection. This suggested that low levels of enzyme release and re-uptake were likely required to achieve metabolic cross-correction in vivo. First, aggressive immunosuppressive preconditioning is required to achieve effective engraftment in the transplanted patients, leading to high morbidity and, in some cases, mortality. These deleterious effects can be severe and may lead to clinical complications in patients that are worse than the disorders themselves. The availability of cord blood repositories and improved transplant methods have reduced these risks, but the possibility of high morbidity remains. Thus, not only must efficient engraftment be achieved after transplantation, but the procedure must also be undertaken before irreversible damage sets in. Because the liver is a natural secretory organ, the concept underlying liver transplantation is that even partial repopulation of this organ with healthy cells will lead to secretion of these proteins into the circulation and widespread metabolic cross-correction. In general, enzymes with terminal sialic acid residues had longer half-lives in the circulation than those with exposed mannose or M6P residues. In the 1980s, a small biotechnology company took on this challenge and began to commercially prepare -glucocerebrosidase, the enzyme deficient in Gaucher disease, from human placentas.
Typically, the hematuria resolves after factor infusion, but if persistent, then a short course of prednisone may prove helpful to shorten the course of hematuria pain treatment center connecticut buy probenecid with paypal. Generally, only one joint is involved at a time, although bleeding may develop simultaneously in two or more joints advanced diagnostic pain treatment center new haven cheap generic probenecid canada. The weight-bearing joints are most commonly affected and the knees are the joints most often severely affected visceral pain treatment guidelines buy probenecid 500 mg overnight delivery. However, because of the success of total knee and total hip replacement surgeries, the ankles are the most commonly affected joints that lead to chronic problems that interfere with quality of life for persons with severe hemophilia chronic pain treatment uk order 500mg probenecid with mastercard. Subcutaneous and Intramuscular Hematomas Large ecchymoses and subcutaneous and intramuscular hematomas were common in hemophilia A prior to the use of regular infusion therapy, reflecting the substantial amounts of time patients had factor levels less than 1% of normal pain treatment center orland park probenecid 500 mg without a prescription. With modern treatment protocols designed to keep plasma levels above 1% of normal, and immediate home infusion when a bleeding episode occurs, the frequency of large soft tissue bleeds has decreased dramatically. Such hemorrhages, when not treated promptly, characteristically spread within fascial spaces and dissect deeper structures. When not treated promptly with factor infusion, the bleeding continues; and at the site of origin, the tissue is hard, indurated, raised, and purplish black. From this center, the hemorrhage extends in all directions, with each successive concentric extension less deeply colored. The point of origin of the hemorrhage may be absorbed entirely while the margin is still progressing. Intramuscular and subcutaneous hematomas may produce leukocytosis, fever, and severe pain in the absence of significant discoloration of the overlying skin. Hematomas may produce serious consequences from the compression of vital structures. Bleeding into the tongue, throat, or neck may develop spontaneously and is especially dangerous because it may compromise the airway with surprising rapidity. Peripheral nerve lesions of varying severity are common complications of untreated hemorrhage into joints or muscles. Traumatic Bleeding Patients with coagulation disorders seldom bleed abnormally from small cuts such as razor nicks, reflecting the normal function of platelets, as measured by platelet function tests. All laboratory assays of platelet function are normal in patients with severe hemophilia A. After larger injuries, however, hemorrhage out of proportion to the extent of the injury is characteristic. The bleeding reflects both increased acute bleeding rates beyond what is expected after the trauma, and persistent bleeding as slow continuous oozing occurs for days, weeks, or months. Such traumatic bleeding may be massive and life-threatening unless coagulation replacement therapy is provided by immediate factor infusion. Thus, although hemostasis after an injury or a minor surgical procedure may appear to be adequate, hemorrhage, often of sudden onset and serious proportions, may develop several hours or even days later. This phenomenon apparently occurs because the processes of primary hemostasis are only temporarily effective. Delayed bleeding may occur in patients with mild hemophilia and is a significant hazard after minor surgical procedures, particularly those performed on an outpatient basis, such as tooth extraction and tonsillectomy. Venipuncture, if skillfully performed, is without danger for the person with severe hemophilia, primarily because of the elasticity of the venous walls. If venipuncture is traumatic, digital pressure on the puncture site or a pressure dressing may prevent further complications. Subcutaneous, intracutaneous, and small intramuscular injections seldom produce hematomas if firm finger pressure is maintained for at least 5 minutes. Vaccination using intramuscular injections is acceptable with minimal increase in bleeding risks. Psoas and Retroperitoneal Hematomas Spontaneous hemorrhage into internal fascial spaces and muscles of the abdomen is common in severe hemophilia A,64 reflecting plasma factor levels less than 1% of normal. Bleeding into or around the iliopsoas muscle produces pain of progressively increasing severity and tenderness; when it occurs on the right side, it may closely simulate acute appendicitis. Femoral nerve involvement may be partial or complete, with the development of pain on the anterior surface of the thigh. The psoas sign is Other Clinical Aspects Infants usually are asymptomatic because they are insulated from trauma. Infants of women who are known carriers may be at risk during delivery, and instrumentation during vaginal delivery should be avoided. Currently, the usual standard of care is to avoid testing the infant in utero due to the risks inherent in current techniques available to test the fetus, and to allow normal vaginal delivery with back-up Caesarean section available if any difficulties arise during birth. Typically, hematomas are seen first when children become active, and hemarthroses seldom develop until they begin to walk. Occasionally, evidence of the disorder is not seen until patients reach teenage years or young adult life. Petechiae, which are characteristic of disorders of platelets and blood vessels, are rare in patients with hemophilia but have been noted in severely affected patients during an exacerbation of bleeding. Hemorrhage from the umbilical cord or stump is unusual, but prolonged bleeding after circumcision is common and brought hemophilia to the attention of the ancient Hebrews. Pulmonary and pleural bleeding are uncommon, although mediastinal and pleural shadows have been noted radiographically and presumably originate from fresh or old hematomas. Intraocular hemorrhage is uncommon, but bleeding into the orbit and conjunctiva occurs often. It is not yet clear whether hemophilia protects older hemophilia patients from thromboembolic disorders,68 atherosclerosis,69 or cardiovascular diseases. Despite the lack of stringent prospective clinical studies for this emerging problem of aging patients with severe hemophilia and other medical problems, reviews of current practice and expert opinion on how to treat aging patients with severe hemophilia have been published. Routine clinical laboratory tests (noncoagulation) are normal in patients with hemophilia A. The presence or absence of anemia or of signs of blood regeneration depends on the severity and frequency of bleeding, as in any individual patient. As in other instances of posthemorrhagic anemia, the bone marrow reflects the response to blood loss. With modern therapy using regular factor infusions to maintain adequate plasma factor concentrations to prevent nearly all spontaneous bleeding episodes, a person born with severe hemophilia A can expect to live an essentially normal lifespan. Hypofibrinogenemia,e reptilase time is prolonged,a fibrin(ogen) degradation products levels are increased. The platelet count usually is normal, but may be elevated in the stress reaction to hemorrhage. Hemarthrosis with significant orthopedic disability is rare in patients with coagulation disorders other than hemophilia A or B. In patients with mild forms of the disorder, however, failure to recognize the existence of the disease or to make the correct diagnosis is more likely. Such patients rarely have a history of spontaneous bleeding, and the family history tends to be vague or negative. A history of abnormal bleeding after minor trauma may be difficult to establish due to variability in bleeding. It must be emphasized that individuals with mild hemophilia are still at risk for hazardous hemorrhage after trauma or during surgical procedures. In the mildly affected patient, specific factor assays must be performed to confirm or exclude the diagnosis of hemophilia. A definitive diagnosis is of great importance because specific products are used to treat each of these disorders. Statistically, one would expect a rare family that might carry both genetic disorders; clearly that situation may be problematic to resolve without additional genetic testing. In clinical practice, if the laboratory results do not seem to fit the clinical picture, then most clinicians will repeat the laboratory test, and/or discuss the results with the laboratory personnel. Two-stage methods,75 one-stage methods,76 and micromethods77 are suitable for diagnosis. They require either a supply of plasma from a known individual with severe hemophilia, which is available commercially, or artificial substrate plasma. The World Health Organization makes international standards, but many laboratories purchase commercial secondary standards that are calibrated to the international standard. Under most circumstances, a pool of citrated plasma carefully collected from normal subjects and frozen in individual laboratories also serves as an acceptable standard. Therefore, when borderline values are obtained, the assay should always be repeated. In most series, 10% of patients have detectable levels ChaPtEr 53 Inherited Coagulation disorders correct diagnosis has not been considered and appropriate laboratory studies have not been ordered. Thus, a deep hematoma may be mistaken for a suppurative condition, and surgical drainage may be attempted. Bleeding into a small joint may produce a clinical and radiologic picture suggestive of sarcoma; when larger joints are involved, findings simulate tuberculosis, arthritis, or Perthes disease. Bleeding elsewhere may suggest local causes such as kidney tumor, pulmonary disease, or peptic ulcer. Intra-abdominal bleeding raises particularly serious diagnostic and therapeutic problems in the patient with hemophilia, even when the hemophilia condition has been accurately diagnosed. Thus, hemorrhage into the psoas, when on the right side, may simulate acute appendicitis so closely that, in the opinion of many experienced clinicians, there is no reliable clinical means to differentiate between the two diagnoses. Intraperitoneal hemorrhage and bleeding into and around other viscera may simulate perforating peptic ulcer, bowel obstruction, or virtually any acute intra-abdominal condition. Computed tomography scanning and sonography may be particularly helpful in differentiating between intra-abdominal conditions that require surgical intervention and retroperitoneal and psoas hemorrhages. Unlike hemophilia A, the spontaneous mutation rate is low,17 and most patients with hemophilia B have positive family histories. Milder gene defects such as splice-site or missense mutations result in a dysfunctional protein with some residual activity. However, in contrast with hemophilia A, most of the genetic causes of hemophilia B are not large deletions or inversions; therefore in many patients there is some antigenic protein, and often some low level of function of the mutated protein. The Leyden variant is detection of carriers Detection of heterozygous carriers of hemophilia B involves the same principles and limitations as described for hemophilia A. Carrier detection based on coagulation assay alone usually is more reliable than is the case with hemophilia A. Such molecules lack Ca2+-binding sites and do not undergo conformational changes induced by Ca2+. Rapid carrier testing using allele-specific microarray methods has been described. This may be because of either the relatively mild nature of the disease in many affected individuals, or a lack of recognition by patients of excessive bleeding in response to either physiologic challenge. Specific factor assays are necessary to distinguish between hemophilia A and hemophilia B. Hemophilia A may be easily distinguished from hemophilia B by a specific factor assay. These designations include angiohemophilia, vascular hemophilia, pseudohemophilia, constitutional thrombopathy, and idiopathic prolonged bleeding time. Evaluation of one large kindred revealed variable severity of bleeding symptoms, with some obligate heterozygote carriers being asymptomatic. The disorder is not homogeneous, however, in part because of the multiple physiologic functions played by ta Bl e 5 3. Variation in levels of as much as 20% has been reported with menstrual cycle, with levels lowest in the early follicular phase (before day 7 of the cycle); and levels increase with age, rising 15% for each decade increase in age. Genetic defects associated with these more severe type 1 phenotypes encode amino acid changes that in turn lead to defects in protein expression. Solid symbols indicate family members who experienced severe bleeding, and crosses indicate family members who experienced hemorrhagic deaths. These have included large gene deletions, small gene deletions, frame-shift mutations, splice-site mutations, nonsense mutations, and point mutations. Rare cases of type 2A disease are transmitted in an autosomal recessive fashion, as are most cases of type 2N disease. This response is highly predictable and is discussed in a later section concerning replacement therapy for hemophilia A. Various hypotheses have been advanced to explain the disproportionate response to transfusion described above. One goal of applying a series of laboratory evaluations is to exclude other causes of bleeding. Even with the more elaborate confirmatory tests now available, the diagnosis of this disorder may be difficult and may require repeated observations over a period of time. Evaluation of a patient at a time remote from acute infection, pregnancy, or strenuous activity is preferable. However, pregnancy and acute-phase reaction are unlikely to obscure diagnosis in patients with more severe quantitative deficiency or qualitative defects. Petechiae are rare, but hematoma formation and the extent of bruising are excessive compared with the inciting trauma. Bleeding manifestations tend to be more prominent in patients with more severe quantitative deficiency and in patients with qualitative (type 2) defects. While eliciting the history of bleeding, one should bear in mind that women are often inaccurate assessors of whether their menstrual flow is normal or excessive. Supplemental questioning regarding the frequency of changes of menstrual protection, and questions regarding a history of iron deficiency anemia and transfusion, may be informative. The physician should specifically seek a history of the response to hemostatic challenge, such as dental extraction, tonsillectomy, surgical procedures, menstruation, peripartum hemorrhage, and transfusion.

The most completely studied antibodies are those that develop in response to quinidine/quinine and heparin swedish edmonds pain treatment center cheap probenecid 500 mg mastercard. Most of the drug-induced antibodies are developed in response to the parent drug, and drug-dependent antibodies can be demonstrated in a variety of in vitro tests advanced diagnostic pain treatment center ct generic 500 mg probenecid with visa. Some patients do not develop thrombocytopenia for months or years, a characteristic that seems to be more dependent on the host than the type of drug chronic pain treatment guidelines 2013 purchase genuine probenecid on line. The amount of drug that is required to cause thrombocytopenia is quite variable; however, even the amount of quinine present in a gin and tonic (15 mg) is sufficient to produce severe thrombocytopenia and bleeding in a patient who has been previously sensitized to quinine ("cocktail purpura") coccyx pain treatment physiotherapy 500 mg probenecid fast delivery. Thrombocytopenia induced by gold salts resolves more slowly, usually over weeks or months, because gold remains in the tissues midsouth pain treatment center germantown tn buy probenecid on line. Although it may be possible to demonstrate drug-dependent antibodies against the parent drug or its metabolites, this type of testing is beyond the scope of hospital laboratories. The readministration of the suspected drug in an attempt to confirm an etiologic relationship is not recommended as a routine diagnostic measure. A detailed history, including all prescribed drugs, over-thecounter medications, and any herbal supplements, is of great benefit. Complete data from all English-language articles describing patients with assumed drug-induced thrombocytopenia have been catalogued on the Internet. Treatment Ordinarily, no therapy is needed, because withdrawal of the offending drug is followed by recovery. Many patients are treated with corticosteroids, and a normal platelet count is usually restored within 1 week. The major exception is goldinduced thrombocytopenia, which may persist for weeks or even months. British anti-Lewisite (dimercaprol) may accelerate the excretion of gold and speed recovery. The candidate drug preceded thrombocytopenia, and recovery from thrombocytopenia was complete and sustained after the drug was discontinued. The candidate drug was the only drug used before the onset of thrombocytopenia, or other drugs were continued or reintroduced after discontinuation of the candidate drug with a sustained normal platelet count. Antibodies against drug metabolites have been reported with acetaminophen, para-aminosalicylic acid, naproxen, and trimethoprim-sulfamethoxazole. Clinical Features Drug-induced thrombocytopenia is associated with a heterogeneous clinical picture and varying degrees of bleeding. Mucosal membrane bleeding from all sites and oral hemorrhagic bullae may occur, and patients often develop fever, chills, nausea, vomiting, and fatigue as part of a prodrome to the bleeding. Thus, as a consequence of the inheritance by the fetus of platelet antigens lacking in the mother, alloantibodies are formed in the maternal circulation and cross the placenta, producing thrombocytopenia in the fetus. However, not all mothers who are missing the antigens presented by the fetus develop antibodies, and not all fetuses and neonates develop thrombocytopenia in spite of antibody development. Platelet counts may or may not normalize with treatment directed only at Helicobacter. It has also been reported in patients with other lymphoproliferative disorders including Hodgkin disease. Platelet-associated IgG has been increased when studied,406 but there may also be an element of enhanced reticuloendothelial phagocytosis. Thrombocytopenia usually is present at birth, but the platelet count may fall further during the postpartum period. Intracranial hemorrhage occurs in 20% to 30%, with one half of the episodes occurring in utero. Maternal plasma should be studied with paternal or neonatal platelets as targets; maternal (antigen-negative) platelets and paternal plasma are appropriate negative controls. Maternal platelets are usually obtained by pheresis, concentrated, irradiated, and transfused. In the absence of any intervention, thrombocytopenia in the second affected fetus is always as or more severe than in the previous fetus/infant. This is a frequently encountered problem in patients who have received multiple platelet transfusions. Pathophysiology and management of chronic immune thrombocytopenia: focusing on what matters. Traditional and new approaches to the management of immune thrombocytopenia: issues of when and who to treat. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. High risk of severe bleeding in aged patients with chronic idiopathic thrombocytopenic purpura. Intravenous anti-D treatment of immune thrombocytopenic purpura: experience in 272 patients. Intravenous anti-D treatment of immune thrombocytopenic purpura: analysis of efficacy, toxicity and mechanism of effect. Systemic review: efficacy and safety of rituximab for adults with idiopathic thrombocytopenic purpura. Variable patterns of response to rituximab treatments in adults with chronic idiopathic thrombocytopenic purpura. Effect of eltrombopag on platelet counts and bleeding during the treatment of chronic idiopathic thrombocytopenic purpura: a randomised, double-blind, placebo-controlled trial. Efficacy of romiplostim in patients with chronic immune thrombocytopenic purpura: a double-blind, randomised controlled trial. Evaluation of bone marrow reticulin formation in chronic immune thrombocytopenia patients treated with romiplostim. Novel approaches to management of immune thrombocytopenic purpura: results of recent trials. Management of alloimmune thrombocytopenia: antenatal diagnosis and in utero transfusion of maternal platelets. Neonatal alloimmune thrombocytopenia: detection and characterization of the responsible antibodies by the platelet immunofluorescence test. Fetal and neonatal alloimmune thrombocytopenia: a management algorithm based on risk stratification. Post-transfusion purpura: a report of five patients and a review of the pathogenesis and management. Mechanisms of thrombocytopenia in chronic autoimmune thrombocytopenic purpura: evidence of both impaired platelet production and increased platelet clearance. Autoantibodies against platelet glycoproteins in autoimmune thrombocytopenic purpura: their clinical significance and response to treatment. Prevalence and clinical significance of elevated antiphospholipid antibodies in patients with idiopathic thrombocytopenic purpura. Clinical and therapeutic experience in 712 Israeli patients with idiopathic thrombocytopenic purpura. Diagnosis and treatment of idiopathic thrombocytopenic purpura: recommendations of the American Society of Hematology. Duration and morbidity of newly diagnosed idiopathic thrombocytopenic purpura in children: a prospective Nordic study of an unselected cohort. A prospective, randomized trial of high-dose intravenous immune globulin G therapy, oral prednisone therapy, and no therapy in childhood acute immune thrombocytopenic purpura. Randomized trial of intravenous immunoglobulin G, intravenous anti-D, and oral prednisone in childhood acute immune thrombocytopenic purpura. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Bellucci S, Charpak Y, Chastang C, Tobelem G, and the Cooperative Group on Immune Thrombocytopenic Purpura. Intravenous gammaglobulin has no advantages over oral corticosteroids as primary therapy for adults with immune thrombocytopenia: a prospective randomized clinical trial. Intravenous gamma globulin treatment for chronic idiopathic thrombocytopenic purpura in children. Intravenous immunoglobulin treatment of chronic idiopathic thrombocytopenic purpura. A multicenter study of the treatment of childhood chronic idiopathic thrombocytopenic purpura with anti-D. It is believed that thrombocytopenia results from consumption of platelets, whereas erythrocyte fragmentation and hemolysis are due to mechanical injury of the red blood cells by abnormal levels of shear stress. Fragmentation of the red blood cells occurs in two types of clinical conditions: vascular devices such as prosthetic heart valves, ventricular assist devices, and extracorporeal oxygenator and microvascular stenosis. In the absence of mechanical devices, fragmentation of the red blood cells signifies stenosis in the arteriolar microvasculature. This is because wall shear stress, determined by blood viscosity, flow rate, and the inverse of the luminal diameter to the third order, is at its highest in the arterioles and may be further increased to exceed the threshold level of red cell fragmentation when the lumen is narrowed. Furthermore, the red cells are likely to be entrapped in the presence of microvascular stenosis. The combination of abnormal shear stress and cell entrapment accounts for red cell fragmentation in patients with arteriolar stenosis. Due to their lower shear stress profile, it is unusual that stenosis in the venules, veins, or arteries is sufficient to cause red cell fragmentation. A comprehensive classification of microangiopathic disorders is listed in Table 48. Thrombotic microangiopathy may also lead to tissue edema and organ dysfunction by increasing vascular permeability. Fibrinoid necrosis and vascular or perivascular inflammatory cell infiltration are characteristically absent or minimal. ChaPtEr 48 Thrombotic Thrombocytopenic Purpura, Hemolytic-Uremic Syndrome, and Related Disorders In chronic cases, the thrombi may be infiltrated by fibroblasts or converted to subendothelial deposits by proliferating endothelial cell lesions. Pseudoaneurysmal dilatation may also be present upstream of the stenosis or occlusion. The ultra-large multimers are depleted and the large multimers are further decreased or depleted in patients presenting with extensive thrombosis and severe thrombocytopenia (lane 3). Lane 3: the ultra-large multimers are depleted and the large multimers are further decreased in patients presenting with extensive thrombosis and severe thrombocytopenia. It is believed that the exosite binding 1 occurs constitutively, whereas exosite binding 2 occurs only when the sequence in the A2 domain downstream of the scissile bond Tyr1605-Met1606 is exposed by shear stress. One mutation, 4143insA, has been detected in at least 15 patients in central-northern Europe, Turkey, and Australia that appear to share a common haplotype. Thrombotic Thrombocytopenic Purpura without Microangiopathic Hemolysis or Thrombocytopenia Thrombocytopenia and microangiopathic hemolysis are not invariably present at the time of acute presentation. Milder cases may present with thrombotic complications or have their disease recognized later in their life. Occasionally, serious complications such as seizures and mental obtundation may occur. The symptoms typically improve immediately after blood transfusion or exchange transfusion performed unknowingly for thrombocytopenia or hyperbilirubinemia. Consequently, the neonates may be discharged from the hospital without a correct diagnosis, only to present with complications of the disease weeks or years later. Others have no or only subtle symptoms and maintain normal or mildly subnormal platelet counts and develop more serious complications only intermittently. The severity may also vary during the lifetime of individual cases, with or without apparent exacerbating conditions such as pregnancy. The thrombotic process may cause focal neurologic deficits, seizures, pancreatitis, or renal failure. Chronic renal failure occurs in approximately 10% of the patients not being regularly treated with plasma infusion, likely a result of cumulative microinfarcts in the kidney. Thrombocytopenia is detectable when platelet consumption exceeds compensatory platelet production. Neurologic complications typically, albeit not invariably, present later, when thrombocytopenia is profound and microangiopathic hemolysis is evident. Most of the patients have no other significant medical history and begin to notice ill-defined symptoms such as headache, dizziness, and fatigue that are often considered insignificant until more serious complications such as profound fatigue, focal neurologic deficits, syncope, mental status changes, or seizures ensue. Less frequently, a patient may present with abdominal pain, nausea, and vomiting, with or without pancreatitis, or chest pain due to myocardial infarction, or even sudden death. In chronic cases, hemolytic anemia may predominate, as active platelet consumption is masked by compensatory thrombopoiesis. It is speculated that in such cases the macrovascular thrombosis may result from thrombotic injury of the vasa vasorum. Occasionally thrombosis may affect large coronary arteries leading to myocardial infarction. Electromechanical dissociation, heart failure, or pulmonary infiltrates or hemorrhage occur in advanced, pre-terminal cases. This assay is technically demanding and not practical for use in clinical laboratories. This explains why the response to plasma therapy may be unsteady for weeks to months and why it is important to monitor the blood counts closely after plasma exchange therapy is tapered. Plasma infusion has the advantage that it does not require a large venous catheter and special equipment. Plasma infusion is used primarily as an emergent substitute until plasma exchange is instituted. Most patients require fresh-frozen plasma every 2 weeks to achieve and maintain normal platelet counts and prevent acute exacerbations. Some patients develop refractory disease after years of quiescent periods or several sporadic relapses. The major side effects of rituximab include allergic reaction and reactivation or exacerbation of viral infections such as hepatitis B and progressive multifocal leukoencephalopathy.
Generic 500 mg probenecid overnight delivery. Hammertowne / Heartaches And Pain.
References
- Yusuf S, Mehta SR, Chrolavicius S, et al; Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators: Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med 2006;354:1464-1476.
- Jing ZC, Xu XQ, Han ZY, et al. Registry and survival study in chinese patients with idiopathic and familial pulmonary arterial hypertension. Chest. 2007;132:373-379.
- Kumral E, Afsar N, Kirbas D, et al. Spectrum of medial medullary infarction: clinical and magnetic resonance imaging findings. J Neurol 2002;249(1):85-93.
- Lupton EW, George NJ: The Whitaker test: 35 years on, BJU Int 105(1):94n100, 2010.
- ZOLL PM: Resuscitation of the heart in ventricular standstill by external electric stimulation, N Engl J Med 247:768-771, 1952.
- Selby WL, Nance KV, Park HK. CEA immunoreactivity in metastatic malignant melanoma. Mod Pathol 1992;5(4):415-9.