
"Cheap nizoral 200mg on-line, antifungal natural shampoo".
K. Randall, M.A.S., M.D.
Co-Director, Texas Tech University Health Sciences Center School of Medicine
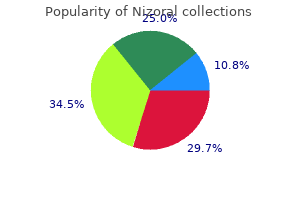
About three fourths of all kidney stones are composed of calcium oxalate: 35% of stones are pure calcium oxalate (calcium oxalate monohydrate or calcium oxalate dihydrate or both); 40% are calcium oxalate with hydroxyapatite or carbonate apatite; and 1% are calcium oxalate with uric acid antifungal antibacterial dog shampoo nizoral 200 mg without a prescription. The non-calcium-containing crystal types are struvite and comprise 8% of all stones fungus anatomy discount nizoral 200 mg overnight delivery, although carbonate apatite is always intermixed in the struvite stone antifungal for cats generic 200 mg nizoral. Eight per cent of all stones are composed of uric acid and 2% are composed of cystine antifungal deodorant order 200 mg nizoral visa. Rarely, stones composed of acid ammonium urate or xanthine or proteinaceous matrix of potentially insoluble drugs are observed. Determining the composition of stones requires polarization microscopy, radiologic diffraction, or infrared spectrometry. The latter two procedures surpass microscopy in precision and sensitivity but are more costly. Formation of kidney stones results from (1) initial formation of crystals (nucleation), (2) reduced effects of normal urinary constituents that inhibit crystal growth and aggregation, (3) the presence of substances promoting crystal growth and aggregation, and (4) the processes that determine crystal attachment to the surface of renal papillary epithelial cells. Attachment allows time for crystal growth and/or aggregation to the size of a clinically symptomatic stone in high urinary solute concentrations. Much of the current approach to evaluating, treating, and preventing nephrolithiasis is centered on identifying excessive urinary excretion of salts that precipitate (nucleate) when units of metastable supersaturation are exceeded (Table 114-2). Supersaturation can result from (1) too little urine output; (2) an absolute increase in the amount of stone constituent excreted over a period of time, such as calcium, oxalate, or uric acid; or (3) altered urine pH. Although most recurrent stone formers tend to have an increased risk of nucleation, 1% or more of stone formers exhibit no detectable abnormality. Many healthy subjects, patients with cancer, and normal pregnant women exhibit hypercalciuria but do not form kidney stones. Thus, factors beside supersaturation are crucial in the pathogenesis of kidney stones. Macromolecular inhibitors of crystal growth and aggregation, particularly the growth and aggregation of calcium oxalate, have been identified (see Table 114-2). Nephrocalcin is a powerful inhibitor of calcium oxalate crystal growth and appears to act by binding to crystal surfaces. This substance is apparently defective when isolated from the urine of calcium stone formers. Urinary osteopontin (uropontin) is perhaps the most potent calcium oxalate crystal growth inhibitor, and its post-translational modifications may be affected in nephrolithiasis because its rate of excretion appears normal. Tamm-Horsfall mucoprotein may inhibit crystal growth but at times promotes calcium oxalate crystal aggregation. Some patients with recurrent nephrolithiasis produce Tamm-Horsfall mucoprotein that self-aggregates and loses its ability to inhibit aggregation of calcium oxalate crystals. Crystal attachment to epithelial surfaces is also crucial for forming at least some stones. Louis, Missouri, from 1987 to 1992 were evaluated with a standardized approach described in the text section on preventing recurrent nephrolithiasis. In addition, there exist specific calcium oxalate crystal receptors on renal tubular epithelial cells. After low urinary volumes, hypercalciuria is the most frequently observed abnormality of the urine from stone formers. In general, the normal upper limit for urinary calcium is 4 mg of calcium per kilogram of body weight per day (280 mg/day, males; 240 mg/day, females) on a diet containing 1000 mg of calcium per day. Total excretion may drop to 200 mg/day on a diet of 400 mg of calcium and 100 mEq or less of sodium. Dietary sodium is important because calcium reabsorption parallels that of sodium in the proximal nephron, such that high rates of sodium excretion are calciuric. Hypercalciuria can result from (1) enhanced absorption from dietary intake; (2) primary renal transport defects leading to excess calcium excretion and secondary enhanced calcium absorption; (3) excessive resorption from storage in bone; or (4) a combination of the above (Table 114-3). Since the late 1980s, a consensus has emerged that the hypercalciuria of nephrolithiasis is a more uniform defect than was previously thought. The basis for this change is the fact that hypercalciuria is the most frequent abnormality found in patients with a family history of nephrolithiasis, suggesting a genetic basis for hypercalciuria. In addition, it has been found that fasting hypercalciuria, observed in 20 to 30% of patients who have nephrolithiasis and hypercalciuria, is not due to a renal transport defect (renal leak) as previously thought. The source of fasting hypercalciuria has been shown to be bone and in many patients is associated with a decrease in bone mineral density.
Levels of most circulating androgens quinine fungus nizoral 200mg fast delivery, especially testosterone fungus fingernail generic nizoral 200 mg amex, tend to be mildly elevated fungus gnats tiny black bugs with wings effective nizoral 200mg. The aim of the diagnostic evaluation is to rule out any causes (such as neoplasms) that require definitive therapy anti fungal anti bacterial ointment trusted 200 mg nizoral. Patients generally require therapy for hirsutism, for induction of ovulation if pregnancy is desired, and for prevention of estrogen-induced endometrial hyperplasia and 1338 cancer. No ideal therapy exists, but rather the therapeutic approach must be individualized to the needs of each patient. In the anovulatory woman not desiring pregnancy who is not hirsute, therapy with intermittent progestin administration (such as medroxyprogesterone acetate, 5 to 10 mg orally for 10 to 14 days each month) or oral contraceptives can be provided to reduce the increased risk of endometrial carcinoma that is present in such a woman with unopposed estrogen. All women utilizing intermittent progestin administration should be cautioned about the need for effective contraception if they are sexually active, because these agents do not inhibit ovulation when administered intermittently. The approach to the hirsute anovulatory woman not desiring pregnancy is detailed in Chapter 255. Oral contraceptive agents are the first line of therapy for such women with mild hirsutism and offer protection from endometrial hyperplasia. Surgical treatment is warranted only rarely and only in women in whom all other methods fail, in whom there is a question of an ovarian tumor because of ovarian size or circulating androgen levels, and in whom fertility is not an issue (because of the risk of pelvic adhesions from the surgery leading to infertility). A particularly severely affected subset of women present with marked obesity, anovulation, mild glucose intolerance and high levels of circulating insulin with insulin resistance, acanthosis nigricans, hyperuricemia, and severe hirsutism with markedly elevated circulating androgen levels. These women have hyperthecosis of the ovaries in which the androgen-producing cells in the stromal, hilar, and thecal components of the ovaries are increased greatly in number. Both hyperthyroidism and hypothyroidism are associated with a variety of menstrual disturbances, including dysfunctional uterine bleeding and amenorrhea as a result of alterations in the metabolism of androgens and estrogens. These metabolic changes in turn result in inappropriate steroid feedback and chronic anovulation. A detailed discussion of the diagnosis and treatment of premature ovarian failure. Recognized disorders of folliculogenesis cannot be identified before ovulation begins. The abnormality can be diagnosed by ultrasonography or by the absence of evidence of ovulation when the ovary is viewed at laparoscopy. The disorder is believed to occur infrequently and sporadically and is probably not a significant cause of infertility. In fact, although the syndrome is believed to occur, data to substantiate its existence are only circumstantial (although strongly suggestive) at present. Progesterone secretion in the luteal phase may be reduced in duration (termed luteal phase insufficiency) or in amount (termed luteal phase inadequacy). More rarely the endometrium may be unable to respond to secreted progesterone because of the absence of progesterone receptors. These disorders are believed to represent causes for infertility (because of inability of fertilized ova to implant) in approximately 5% of infertile couples. Abnormalities of the follicular phase, especially in the frequency of gonadotropin pulses, may account for most luteal phase defects. Luteal phase defects also may occur sporadically in normally ovulating women approximately once each year. Luteal phase dysfunction may be associated with several clinical entities, including mild or intermittent hyperprolactinemia (of any cause), strenuous physical exercise, inadequately treated 21-hydroxylase deficiency, and habitual abortion. Luteal dysfunction occurs more commonly at the extremes of reproductive life and in the first menstrual cycles following full-term delivery, abortion, or discontinuation of oral contraceptives. The diagnosis of luteal phase dysfunction can be made either by endometrial biopsy or by serial progesterone determinations. Endometrial biopsies obtained from the uterine fundus in the late luteal phases of two different cycles must be at least 2 days out of phase from the expected date of bleeding, as judged from the subsequent menstrual cycle, for the diagnosis to be made. The absolute concentration that progesterone must achieve and the length of time progesterone must be increased in the luteal phase to exclude luteal dysfunction are unclear. Luteal dysfunction is extremely rare in women with menstrual cycles greater than 25 days in length in whom a single random progesterone determination is greater than 15 ng/mL.
The precise incidence of the disease is not known because it is not reportable; however fungus mold discount 200 mg nizoral mastercard, a reasonable annual estimate for the United States is 400 antifungal cream for feet buy cheap nizoral 200mg,000 bouts of sepsis antifungal therapy order nizoral 200mg online, 200 fungus in hair cheap nizoral 200 mg with amex,000 cases of septic shock, and 100,000 deaths from this disease. Compared with gram-positive organisms, gram-negative bacteria are somewhat more likely to produce septic shock. Culture-positive gram-negative bacteremia produces shock in approximately 50% of infections, whereas gram-positive bacteremia produces shock in about 25% of infections. Frequent causes of sepsis are pyelonephritis, pneumonia, peritonitis, cholangitis, cellulitis, meningitis, or abscess formation at any site. Many of these infections are nosocomial and occur in patients hospitalized for other medical problems. In patients with normal host defenses, a site of infection is identified in most patients. In neutropenic patients, however, a clinical site of infection is found in less than 50% of septic patients, probably because small, clinically inapparent infections in skin or bowel can lead to blood stream invasion in patients with inadequate circulating neutrophils. Definitions have incorporated manifestations of the systemic response to infection (fever, tachycardia, tachypnea, and leukocytosis) as well as evidence of organ system dysfunction (cardiovascular, respiratory, renal, hepatic, central nervous system, hematologic, or metabolic abnormalities). Sepsis is severe and has a poorer prognosis when it is associated with organ dysfunction, hypoperfusion (lactic acidosis, oliguria, or altered mental status), or hypotension (septic shock). Septic shock is defined as sepsis-induced hypotension that persists despite adequate fluid resuscitation and is associated with hypoperfusion abnormalities or organ dysfunction. In clinical practice, many patients with these signs and symptoms are receiving vasopressor and/or inotropic agents and are no longer hypotensive when they manifest hypoperfusion abnormalities or organ dysfunction, but they still are considered to be experiencing septic shock. These organism-derived products can stimulate the release of a large number of endogenous host-derived mediators from plasma protein precursors or cells (monocytes-macrophages, endothelial cells, neutrophils, and others). The endogenous mediators can produce profound physiologic effects on the vasculature and organ systems. When released in small amounts, these mediators result in beneficial effects such as regulating immune function, killing bacteria, and detoxifying bacterial products. Systemic inflammatory response syndrome: the systemic inflammatory response to a variety of severe clinical insults. The response is manifested by two or more of the following conditions: Temperature >38РC or <36РC Heart rate >90 beats/min Respiratory rate >20 breaths/min or Pa co2 <32 mm Hg (<4. This systemic response is manifested by two or more of the following conditions as a result of infection: Temperature >38РC or <36РC Heart rate >90 beats/min Respiratory rate >20 breaths/min or Pa co2 <32 mm Hg (<4. Hypoperfusion and perfusion abnormalities may include, but are not limited to , lactic acidosis, oliguria, or an acute alteration in mental status. Septic shock: Sepsis with hypotension, despite adequate fluid resuscitation, along with the presence of perfusion abnormalities that may include, but are not limited to , lactic acidosis, oliguria, or an acute alteration in mental status. Patients who are on inotropic or vasopressor agents may not be hypotensive at the time that perfusion abnormalities are measured. Hypotension: A systolic blood pressure <90 mm Hg or a reduction >40 mm Hg from baseline in the absence of other causes for hypotension. Multiple organ system failure: Presence of altered organ function in an acutely ill patient such that homeostasis cannot be maintained without intervention. Adapted from American College of Chest Physicians Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Although certain mediators are undoubtedly more important than others in producing sepsis, probably dozens of organism- and host-derived mediators interacting, accelerating, and inhibiting one another are responsible for the pathogenesis of septic shock. Approximately 50% of patients who have hypotension secondary to sepsis and who are admitted to an intensive care unit survive; the other 50% develop refractory hypotension or multiple organ system failure and die from progressive septic shock. Early and throughout the course of most of these patients, cardiovascular evaluation reveals a low systemic vascular resistance and a high cardiac output-the hyperdynamic response to sepsis. Despite this elevated cardiac output, cardiac performance is abnormal, with a decreased ventricular ejection fraction and a dilated ventricle. In approximately 20% of patients, progressively diminished cardiac performance results in an abnormally low cardiac output. Death results from progressive hypotension or complete failure of one or more organ systems. Certain microorganisms synthesize and release exotoxins that can activate the cascade. More frequently, the structural components of the microorganism initiate the sequence.
Syndromes
- Chemical irritation - from almost any fluid that gets into the eye
- Fragrances in perfumes, cosmetics, soaps, and moisturizers
- Drug therapy to suppress the immune system
- Congenital (present at birth) valve problems, such as bicuspid valve
- Paroxysmal supraventricular tachycardia
- Concussion
These patients not only rapidly clear transfused platelets from their circulation but also destroy their own platelets and become thrombocytopenic usually 5 to 10 days after transfusion fungus gnats bananas buy nizoral 200 mg free shipping. Thrombocytopenia caused by maternal alloantibodies against fetal platelet antigens occurs in approximately 1 in 2000 to 4000 fetuses antifungal keratosis pilaris buy cheap nizoral 200mg line. Affected infants may have intracranial hemorrhage (estimated at between 10 and 30%); in families with an affected infant fungus gnats fox farm order nizoral 200mg visa, the risk of recurrence is at least 75% antifungal rinse order 200mg nizoral fast delivery. Women with a prior history of an affected infant should give birth by cesarean section. Alteration in the integrity or structure of blood vessels can lead to a bleeding diathesis, the symptoms and signs of which are indistinguishable from those of a platelet disorder. This disorder, the most common genetic cause of vascular bleeding, is inherited as an autosomal dominant trait. More than half of these patients have epistaxis by 20 years of age and 90% by age 45. Telangiectasia occurs most frequently on the face in two thirds of patients, on the mouth in half, and on the cheeks, tongue, nose, and lower lip in approximately one third. Beyond this cutaneous or mucosal involvement, the organ system affected most often is the gastrointestinal tract (15%). Death from intestinal bleeding occurs in 12 to 15% of patients with symptomatic gastrointestinal involvement. The liver, lungs, central nervous system, and urinary tract are involved in decreasing order of frequency. Pulmonary arteriovenous fistulas, present in approximately 5% of patients, are manifested by cyanosis, dyspnea, clubbing, and thoracic murmurs. Stroke may occur with central nervous system involvement, a complication that tends to affect younger patients (mean age, 33 years). Pathologic examination of involved tissue demonstrates dilated capillaries with loss of subendothelial structures. Although no therapy is consistently effective, based on a few case reports and one small series of patients, conjugated estrogen-progestin therapy appears to be efficacious in decreasing the number of bleeding episodes. Congenital subcutaneous and visceral hemangiomas may be associated with thrombocytopenia and bleeding in infants and children. Bleeding occurs at the site of the lesions or systemically secondary to thrombocytopenia. Platelets are activated within the hemangioma and subsequently removed from the circulation. In addition, mild disseminated intravascular coagulation may occur with consumption of fibrinogen. In cases in which thrombocytopenia is severe and tumors are few, surgery and/or radiation therapy may be effective. Intentional thrombosis of hemangiomas by the administration of inhibitors of fibrinolysis, with or without cryoprecipitate, has been successful in managing thrombocytopenia in a few cases. Also, interferon-alpha has been observed to cause significant regression of hemangiomas. Genetic abnormalities in structural glycoproteins such as collagen can result in vascular fragility caused by weakening of the vessel wall. Bleeding may be limited to increased bruising or may be manifested as internal hemorrhaging. Ehlers-Danlos syndrome (see Chapter 216), osteogenesis imperfecta (see Chapter 217), and pseudoxanthoma elasticum (see Chapter 218), are examples of inherited disorders of connective tissue that may be associated with a bleeding diathesis on this basis. Severe vitamin C deficiency results in defective collagen formation in small blood vessels. Bleeding may occur in any tissue but is prominent in the lower extremities and is perifollicular in distribution. Other sites where bleeding is common include the gums, the subperiosteum in children, and muscle. In type I, bleeding may be due to obstruction of blood flow in the microcirculation at cold temperatures by cryoprecipitates, with subsequent increased vascular fragility. In this syndrome, patients have polyclonal hyperglobulinemia associated with purpura of the lower extremities. Leukocytoclastic involvement of the vessel wall may account for the increased vascular fragility and bleeding. Commonly, the onset of purpura is preceded by a stinging sensation in areas of involvement.