
"Safe 100 mg desyrel, anxiety rash pictures".
Y. Ines, M.S., Ph.D.
Associate Professor, California Health Sciences University
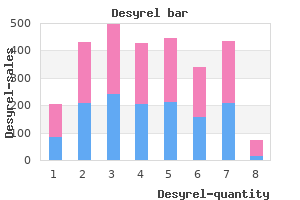
Contraction of gastrointestinal smooth muscle requires an increase in the intracellular calcium concentration anxiety symptoms 6 days buy generic desyrel 100 mg line, which is necessary to phosphorylate the myosin light chain that is required to form cross-bridges with actin anxiety symptoms vs heart attack buy generic desyrel 100mg. When receptors are activated anxiety unspecified 100 mg desyrel with mastercard, inositol triphosphate is produced and releases calcium from the sarcoplasmic reticulum or stimulates opening of voltage-dependent or receptor-operated calcium channels anxiety symptoms medications best desyrel 100 mg. The rapid actin-myosin cross-bridge formation is associated with a rapid increase in the velocity of smooth muscle shortening. Relaxation of smooth muscle is equally important for transporting intraluminal contents through the gastrointestinal tract. Cyclic adenosine monophosphate production, initiated by ligand activation of receptors on the smooth muscle cell membrane, decreases intracellular calcium concentration by moving calcium into sarcoplasmic reticulum or out of the cell. Enteric neurons contain many different excitatory and inhibitory neurotransmitters (Table 132-1), and the complex interaction among inhibitory and excitatory neurotransmitters coordinates bowel activity. The intrinsic enteric neurons of the gastrointestinal tract have numerous interconnections. Input comes from the central nervous system, internuncial neurons, and interaction with afferent neurons by means of the prevertebral ganglia. Sympathetic and cholinergic fibers, which originate in the central nervous system and travel in the vagus, splanchnic, lumbar colonic, or sacral nerves, regulate the output of neurotransmitters from the myenteric plexus. Control of the myenteric plexus is mediated by intestinal afferent neurons and central nervous system neurons, interacting in the celiac, superior mesenteric, and inferior mesenteric ganglia. The interaction of interneurons within the myenteric plexus controls Figure 132-2 Schematic diagram showing control levels for neural regulation of gastrointestinal effector function. The enteric nervous system integrates information from the periphery and the central nervous system and modulates effector function. In prevertebral ganglia, afferent inputs from the gut and descending inputs through the sympathetic branch of the autonomic nervous system are integrated into output that has primarily inhibitory effects on gut motility. Autonomic nuclei of sympathetic and parasympathetic nerves located in the brain stem integrate inputs from the periphery and the cortex. The proximal three ports are in the antrum, port 4 is in the pylorus with contractions at the gastric and duodenal frequencies, and ports 5 through 8 are in the duodenum. A phase 3 migrating motor complex progresses from the stomach (3 cycles/min) down the duodenum (11 cycles/min). Each site of neural interconnection may be a potential target for future therapeutic intervention. Afferent sensory nerves play a large role in the symptoms of abdominal pain or bloating in patients with gastrointestinal motility disorders. Patients with functional gastrointestinal diseases (Chapter 131) have a heightened awareness and decreased threshold for pain perception to esophagogastrointestinal distention but not to stimulation of somatic structures. The visceral hypersensitivity may be due to sensitization of the neurons in the gut, dorsal horn, or thalamus. Peptides, released from the gastrointestinal mucosa into the blood after eating, act as hormones and affect gastric, small intestinal, and colonic smooth muscle contractions. Further flexibility is gained as peptide hormones modulate motility by regional variation in response to a peptide. Blood levels of the enteric hormonal peptides reach their maximum 30 to 60 minutes after eating. Each of the major sections of the gastrointestinal tract has a specific function that requires a different transit pattern. Eating ends the fasting motility pattern and initiates a postprandial transit pattern in each segment of the alimentary tract. Emotional stress and physical exercise modulate these patterns but are not the primary controls. As an initial response to eating, the proximal stomach relaxes to accommodate the volume of a meal. The distal stomach grinds the masticated chunks of food to less than 1 mm diameter and regulates the delivery of the processed gastric contents to the intestine synchronous with the release of digestive enzymes. Gastric emptying adjusts to the different physical and chemical characteristics of the food.
Patients have circulating autoantibodies that not only react against the tumor tissue but also cross-react with similar antigens found in the epidermal cell junction of normal skin anxiety symptoms 8 year old boy discount desyrel 100 mg with visa. A number of miscellaneous dermatoses have been associated with internal malignancies anxiety pictures purchase desyrel 100 mg visa, but it is not entirely clear whether these associations are real or fortuitous anxiety symptoms for no reason order desyrel 100mg without a prescription. Syndromes and Entities Involving the Skin and Internal Malignancies A number of unique cutaneous syndromes are associated with internal neoplasms with sufficient frequency to alert the clinician to look for these tumors when they are potentially curable anxiety games order 100mg desyrel fast delivery. Certain skin lesions have a high prevalence of associated neoplasia, whereas in others the prevalence is low. A breast mass may not be palpable or may not even be found with mammography, but in virtually every case an underlying cancer is found. The lesion mimics eczema, which improves with topical therapy; any eczematous lesion on the nipple that does not respond to topical steroids should undergo biopsy, which shows diagnostic pathologic changes. In this disorder, eczematous, pruritic, crusted, lichenified, well-demarcated patches may involve the lower part of the abdomen, inguinal regions, genitalia, or perianal area. Patients are usually older than 50 years, and an underlying carcinoma of the rectum, prostate, urethra, other parts of the genitourinary tract, or apocrine glands is found in up to 50%. The most common sites of metastasis, when present, are regional inguinal and pelvic lymph nodes, bone, liver, lung, brain, and bladder. Stewart-Treves syndrome is the occasional occurrence of a lymphangiosarcoma as a complication of chronic lymphedema of the arm after radical mastectomy for carcinoma of the breast. Angiomatous, livid, or dusky red blobs and nodules may evolve 2 to 20 years following the onset of postoperative lymphedema. Angiosarcoma has also developed in congenital lymphedema, as well as in lymphedema of the legs following surgery for cervical cancer. Acanthosis nigricans (see color Plate 14 A) is characterized by soft, velvety, verrucous, brown hyperpigmentation with skin tags in the body folds, especially those of the neck, axilla, and groin. When it occurs in patients older than 40 years, it is often a sign of an underlying malignant tumor, usually adenocarcinoma (most often of the stomach, gastrointestinal tract, and uterus; less commonly of the ovary, prostate, breast, and lung; and rarely lymphoma). Acanthosis nigricans involving the tongue and oral mucosa is highly suggestive of an underlying neoplasm. In 80% of cases, the cancer is abdominal; in 60% of cases, the cancer is found in the stomach. Special concern must be given to non-obese adults in whom pigmented verrucous areas have recently developed in the body folds; in 80 to 90%, an underlying gastric cancer is present. Of patients with acanthosis and malignancy, the skin abnormalities precede the appearance of the neoplasm in 20% of cases. The skin findings often regress following successful antitumor therapy and reappear with recurrence of the tumor, which suggests that the underlying tumor secretes an unidentified substance that is responsible 1056 for the verrucoid skin lesions. Dermatomyositis (see Color Plate 14 B) is recognized by proximal muscle pain and weakness and a characteristic dermatitis that includes a heliotrope rash (edematous, violaceous, telangiectatic discoloration of the eyelids) along with a violaceous, erythematous, telangiectatic scaling rash on the cheeks, forehead, V of the neck, elbows, and knees. In individuals older than 40 years, the prevalence of internal carcinoma, primarily breast and lung tumors, is increased (see Chapter 296). Not uncommonly, the dermatomyositis resolves on removal of the carcinoma, but it may recur if the tumor reappears. Neoplasm should be especially suspected if the dermatomyositis does not respond to conventional therapy, if the patient has a history of previous malignant disease, or if atypical symptoms of dermatomyositis are present. The Leser-Tre lat sign, or the sudden or eruptive appearance or increase in size of multiple seborrheic keratoses, occurs with underlying cancer in the elderly. This sign has been the subject of controversy because seborrheic keratoses are common in the elderly, as are cancers, so their simultaneous occurrence may not have any relationship. Nevertheless, several case reports have described new and enlarging keratoses in association with cancer of the lung, adenocarcinoma of the bowel, mycosis fungoides, and Sezary syndrome; in some of these patients, the keratoses regressed when the malignant tumor was treated. Lymphomatoid papulosis is an uncommon condition of cutaneous lymphoid infiltration clinically characterized by involuting and recurring purplish red papules, plaques, and nodules. Based on histologic features, lymphomatoid papulosis has been divided in two types: type A lesions contain large anaplastic tumor cells, whereas type B lesions have cerebriform mononuclear cells and epidermotropism indistinguishable from the changes seen in mycosis fungoides. Unfortunately, no single clinical or pathologic feature distinguishes lymphomatoid papulosis from lymphoma.
Common renal manifestations are albuminuria and renal insufficiency found in almost one half of patients anxiety in teens desyrel 100 mg with amex. Treatment strategies for renal amyloidosis have focused on combined therapy with melphalan anxiety therapy 100mg desyrel overnight delivery, prednisone anxiety symptoms causes quality 100mg desyrel, and colchicine or marrow transplantation and ablative therapy to destroy the clone of abnormal plasma cells leading to the amyloid production anxiety symptoms pregnancy purchase desyrel 100 mg with amex. However, the deposits do not form beta-pleated sheets, do not stain with Congo red, and are granular rather than fibrillar. Moderate albuminuria is common, and the nephrotic syndrome is found in one half at presentation, often accompanied by hypertension and renal insufficiency. Fibrillary Glomerulopathy-Immunotactoid Glomerulopathy Some patients with renal disease have glomerular lesions with deposits of non-amyloid fibrillar proteins ranging in size from 12 to 49 nm. In the past, these lesions were called fibrillary glomerulopathy, immunotactoid glomerulopathy, amyloid-like glomerulopathy, Congo red-negative amyloid-like glomerulonephritis, and non-amyloiditic fibrillary glomerulopathy. Recently, patients with these lesions have been divided into two groups: those with fibrillary glomerulonephritis with fibrils of 20 nm in diameter and those with immunotactoid glomerulonephritis, a rare disease in which the fibrils are much larger (30 to 50 nm). Proteinuria is found in almost all patients, and hematuria, the nephrotic syndrome, and renal insufficiency are eventually found in the majority. There are severe tubulointerstitial changes with interstitial inflammation, edema, microcystic dilatation of tubules, and severe tubular degenerative changes. Mixed Cryoglobulinemia Cryoglobulinemia is caused by the production of circulating immunoglobulins that precipitate on cooling and resolubilize on warming. Recently, many patients with what was originally described as glomerulonephritis due to essential mixed cryoglobulinemia have been found to have hepatitis C-associated renal disease. Most patients have proteinuria, and about 20% present with the nephrotic syndrome. The majority with renal disease have a slow, indolent renal course characterized by proteinuria, hypertension, hematuria, and renal insufficiency. Hypocomplementemia, especially of the early components Clq-C4, is a characteristic and often helpful finding in cryoglobulinemic glomerulonephritis. Thrombotic Microangiopathies A number of systemic diseases including hemolytic-uremic syndrome, thrombotic thrombocytopenic purpura, and the antiphospholipid syndrome (see Chapter 184), as well as microangiopathy associated with drugs such as mitomycin and cyclosporine are characterized by microthromboses of the glomerular capillaries and small arterioles. The renal findings may be dominant or only part of a more generalized picture of microangiopathy. Glomerular capillary thromboses are noted in some glomeruli, whereas others downstream from thrombosed arterioles may show only ischemic damage. Arterioles and small arteries show intimal proliferation with luminal narrowing by thrombus. The renal manifestations of the thrombotic microangiopathies may include gross or microscopic hematuria, proteinuria that is typically less than 2 g/day but may reach nephrotic levels, and renal insufficiency. Treatment of the thrombotic microangiopathies includes correcting hypovolemia, controlling hypertension, and use of dialytic support for those with severe renal failure. In the antiphospholipid syndrome, anticoagulation with heparin and then warfarin (Coumadin) has been useful. The renal lesions of these disorders typically range from focal and segmental necrotizing glomerulonephritis to severe necrotizing crescentic glomerulonephritis. A review of the epidemiology, pathogenesis, clinical features, course, and treatment of this increasing form of idiopathic nephrotic syndrome. A controlled trial of three treatment regimens for lupus nephritis emphasizing renal survival as an outcome and the side effects of therapy. A review of the patterns of kidney involvement by hepatitis C including data on therapy with interferon. An analysis of clinical features and response to therapeutic regimens of 220 patients with primary amyloidosis. Maschio G, Alberti D, Janin G, et al: Effect of the angiotensin-converting enzyme inhibitor benazepril on the progression of chronic renal insufficiency. A review of the features, pathophysiology, and treatment of the various patterns of the nephrotic syndrome. Schieppati A, Mosconi L, Perna A, et al: Prognosis of untreated patients with idiopathic membranous nephropathy. A long-term follow-up of idiopathic membranous nephropathy showing favorable prognosis without specific immunosuppressive therapy. The tubules and interstitium of the kidney are separate structural and functional compartments that are intimately related, and any injury initially involving either of them will inevitably be associated with damage to the other, hence the term tubulointerstitial diseases. A constant histologic feature of these diseases is an inflammatory cell infiltrate.
Syndromes
- Seizures
- Falls, drownings, and other accidents
- Echinococcus
- Osteogenesis imperfecta
- Try not to scratch the area.
- STD tracking
- Choking
- Need for more breast surgery
Comprehensive description of pathogenesis and clinical description of this important cause of hypercholesterolemia anxiety symptoms gerd buy 100 mg desyrel otc. Comprehensive and current concepts of metabolism of apo B-containing lipoproteins anxiety symptoms chest pains generic desyrel 100mg visa. Most comprehensive and up-to-date discussion of role of apo E in lipoprotein metabolism papa roach anxiety order 100mg desyrel amex. Easy-to-read book covering both basic research and clinical aspects of lipoprotein metabolism and their relationship to atherosclerosis anxiety in college students purchase desyrel 100mg with amex. Over 40 single base changes have been identified within the coding region, as well as several deletions and splicing mutations leading to loss of enzymatic activity. The great majority of affected individuals are heteroallelic for two different molecular defects. The pathogenesis of this disorder and its selectivity for cells of the immune system have been the subject of considerable interest. Other pathogenic mechanisms that may play a role in the selective lymphocytotoxicity include inhibition of the enzyme S-adenosylhomocysteine hydrolase by 2 -deoxyadenosine, which results in a decrease in transmethylation reactions mediated by S-adenosylmethionine, and a direct toxic effect of adenosine on lymphocytes mediated by adenosine receptors. Pneumocystis carinii infections and candidiasis are commonly observed, as well as cytomegalovirus, varicella, and other viral pneumonias and infections. Vaccination with live organisms may be fatal, and an increased incidence of B-cell lymphomas has been reported. Recurring respiratory infections may lead to pulmonary insufficiency in older individuals. Physical findings are unremarkable with the exception of an absence of lymph nodes and tonsillar tissue and the presence in some affected infants of very prominent costochondral junctions. Neurologic abnormalities have been reported in occasional cases, as have autoimmune abnormalities such as hypothyroidism, hemolytic anemia, and immune thrombocytopenic purpura. Chest radiographs reveal the absence of a thymus, and peripheral blood examination usually demonstrates an absolute lymphopenia of less than 500/muL with a marked reduction in mature T cells and a more variable decrease in B cells associated with hypogammaglobulinemia and lack of specific antibody response to immunization. In vitro tests of lymphocyte function, including proliferative responses to mitogens and antigen, are abnormal. The disorder should be looked for in individuals with recurrent infections associated with unexplained lymphopenia. Haploidentical transplants with T-cell-depleted marrow have been less successful, with the probability of long-term survival rates ranging from 28 to 67%. Although lymphocyte counts do not return to normal, the majority of patients have a major reduction in infectious episodes and have resumed growth and normal activities. The future success of the gene therapy approach will depend on the development of improved vectors that enable higher transduction efficiencies. Neurologic abnormalities, including spasticity, ataxia, behavioral abnormalities, and hypertonia or hypotonia, have been observed in over 50% of affected individuals. Patients are generally seen in childhood with recurrent infections associated with markedly reduced T-lymphocyte counts and are found to lack a thymus gland on chest radiography. Only 2 of 8 patients have had long-term engraftment following bone marrow transplantation. It is manifested as a devastating neurologic disorder consisting of compulsive self-mutilation, choreoathetosis, spasticity, and often mental retardation. The syndrome occurs at a frequency of 1 in 100,000 births and is associated with a marked overproduction of purines resulting in hyperuricemia and gout (see Chapter 299). Partial deficiency of the enzyme also causes hyperuricemia, but without severe neurologic deficits, and accounts for fewer than 1% of patients with gout. In addition, an increase in the intracellular concentration of phosphoribosylpyrophosphate and reduced formation of inosine and guanine monophosphate lead to a marked increase in the overall rate of de novo synthesis of purine nucleotides, further increasing the generation of uric acid. The clinical sequelae of hyperuricemia and increased uric acid excretion are the juvenile onset of uric acid stone formation and gouty arthritis. The pathogenesis of the neurologic defects is not completely understood but could involve guanine nucleotide deficiency as a result of decreased guanine salvage in neurons that depend on the salvage pathway for purine nucleotide synthesis. Positron emission tomography has demonstrated a selective decrease in dopamine transporters of 50 to 70% in the caudate and putamen. Although anatomic studies of the brains of affected individuals have not revealed any structural lesions, imaging studies have revealed a significant reduction in caudate volume. The Lesch-Nyhan syndrome is manifested in affected males during the 1st year of life by an initial delay in motor development, followed by extrapyramidal signs leading to choreoathetosis and, at approximately age 1, by pyramidal tract involvement with hyperreflexia, clonus, and scissoring of the legs.